From Surf Wiki (app.surf) — the open knowledge base
Urinary tract infection
Infection that affects part of the urinary tract
Infection that affects part of the urinary tract
| Field | Value |
|---|---|
| name | Urinary tract infection |
| image | Pyuria.JPG |
| caption | Multiple white cells seen in the urine of a person with a urinary tract infection using microscopy |
| field | Infectious disease Urology |
| synonyms | Acute cystitis, simple cystitis, bladder infection, symptomatic bacteriuria |
| symptoms | Pain with urination, frequent urination, cloudy urine, feeling the urge to urinate despite having an empty bladder |
| causes | Most often E. coli bacteria |
| risks | Catheterisation (foley catheter), female anatomy, sexual intercourse, diabetes, obesity, family history |
| diagnosis | Based on symptoms, urine culture |
| differential | Vulvovaginitis, urethritis, pelvic inflammatory disease, interstitial cystitis, kidney stone disease |
| treatment | Antibiotics |
| frequency | 405 million (2019) |
| deaths | 260,000 (2021) |
A urinary tract infection (UTI) is an infection that affects a part of the urinary tract, which includes the bladder, urethra and the kidney. Lower UTIs affect the bladder (cystitis) or urethra while upper UTIs affect the kidney (pyelonephritis). Symptoms from a lower UTI include burning or pain during urination, pain in the lower abdomen and the urge to urinate even when the bladder is empty. Symptoms of a kidney infection are more systemic and include fever or flank pain, usually in addition to the symptoms of a lower UTI. Rarely, the urine may appear bloody. Symptoms may be less clear in very young or old people.
The most common cause of infection is E. coli, though other bacteria or fungi may sometimes be the cause. Risk factors include being female, sexual intercourse, diabetes, using a catheter, and family history. Kidney infections usually occurs when a bladder infection spreads, but may also come from bacteria in the blood. Diagnosis in young healthy women can be based on symptoms alone. In those with vague symptoms, diagnosis can be harder because bacteria may be present even if there is no infection.
In uncomplicated cases, UTIs are usually treated with a short course of antibiotics. Resistance to many of the antibiotics used to treat this condition is increasing. In complicated cases, a longer course or intravenous antibiotics may be needed. If symptoms do not improve in two or three days, further diagnostic testing may be needed. People with bacteria or white blood cells in their urine but no symptoms usually do not need antibiotics. For people with recurrent infections, methenamine may be prescribed. Postmenopausal women may also be offered vaginal estrogen replacement. If these do not work, preventative antibiotics can be considered.
Approximately 400 million UTI cases occur each year. Up to 10% of women have a urinary tract infection in a given year, and half of women have at least one infection at some point in their lifetime. They occur most frequently between the ages of 16 and 35years. Recurrences are common. Urinary tract infections have been described since ancient times with the first documented description in the Ebers Papyrus dated to c. 1550 BC.
Signs and symptoms

The most common symptoms of a UTI are burning with urination and having to urinate frequently (or an urge to urinate) in the absence of vaginal discharge and significant pain.
Children
In young children, the only symptom of a urinary tract infection (UTI) may be a fever.
Elderly
Urinary tract symptoms are frequently lacking in the elderly. Some present to a health care provider with sepsis, an infection of the blood, as the first symptoms.
It is reasonable to obtain a urine culture in those with signs of systemic infection that may be unable to report urinary symptoms, such as when advanced dementia is present. Systemic signs of infection include a fever or increase in temperature of more than 1.1 C-change from usual, chills, and an increased white blood cell count.
Cause

Pathogenic E. coli from the gut is the cause of 75% of uncomplicated UTIs, and 65% of complicated UTIs. Rarely they may be due to viral or fungal infections. Healthcare-associated urinary tract infections (mostly related to urinary catheterization) involve a much broader range of pathogens including: Klebsiella pneumoniae, Proteus mirabilis, Pseudomonas aeruginosa and Enterococcus faecalis. These species can form biofilms and colonise catheders. In sub-Saharan Africa, Staphylococcus aureus, which typically occurs secondary to blood-borne infections is more common.
Chlamydia trachomatis and Mycoplasma genitalium can infect the urethra but not the bladder. These infections are usually classified as a urethritis rather than urinary tract infection.
{{anchor|Honeymoon cystitis}}Intercourse
In young sexually active women, sexual activity is the cause of 75–90% of bladder infections, with the risk of infection related to the frequency of sex. Condom use without spermicide or use of birth control pills does not increase the risk of uncomplicated urinary tract infection.
Anal intercourse may increase the risk of UTI in men and in women if followed by vaginal sex.
Although sex is a risk factor, UTIs are not classified as sexually transmitted infections (STIs).
Sex
Women are more prone to UTIs than men because, in females, the urethra is much shorter and closer to the anus. As a woman's estrogen levels decrease with menopause, her risk of urinary tract infections increases due to the loss of protective vaginal flora.
Chronic prostatitis in the forms of chronic prostatitis/chronic pelvic pain syndrome and chronic bacterial prostatitis (not acute bacterial prostatitis or asymptomatic inflammatory prostatitis) may cause recurrent urinary tract infections in males.
Urinary catheters
Urinary catheterization increases the risk for urinary tract infections.
Male scuba divers using condom catheters and female divers using external catching devices for their dry suits are also susceptible to urinary tract infections.
Others
A predisposition for bladder infections may run in families. Other risk factors include diabetes, and having a large prostate. In children UTIs are associated with vesicoureteral reflux (an abnormal movement of urine from the bladder into ureters or kidneys) and constipation.
Persons with spinal cord injury are at increased risk for urinary tract infection in part because of chronic use of catheter, and in part because of voiding dysfunction. It is the most common cause of infection in this population, as well as the most common cause of hospitalization.
Pathogenesis
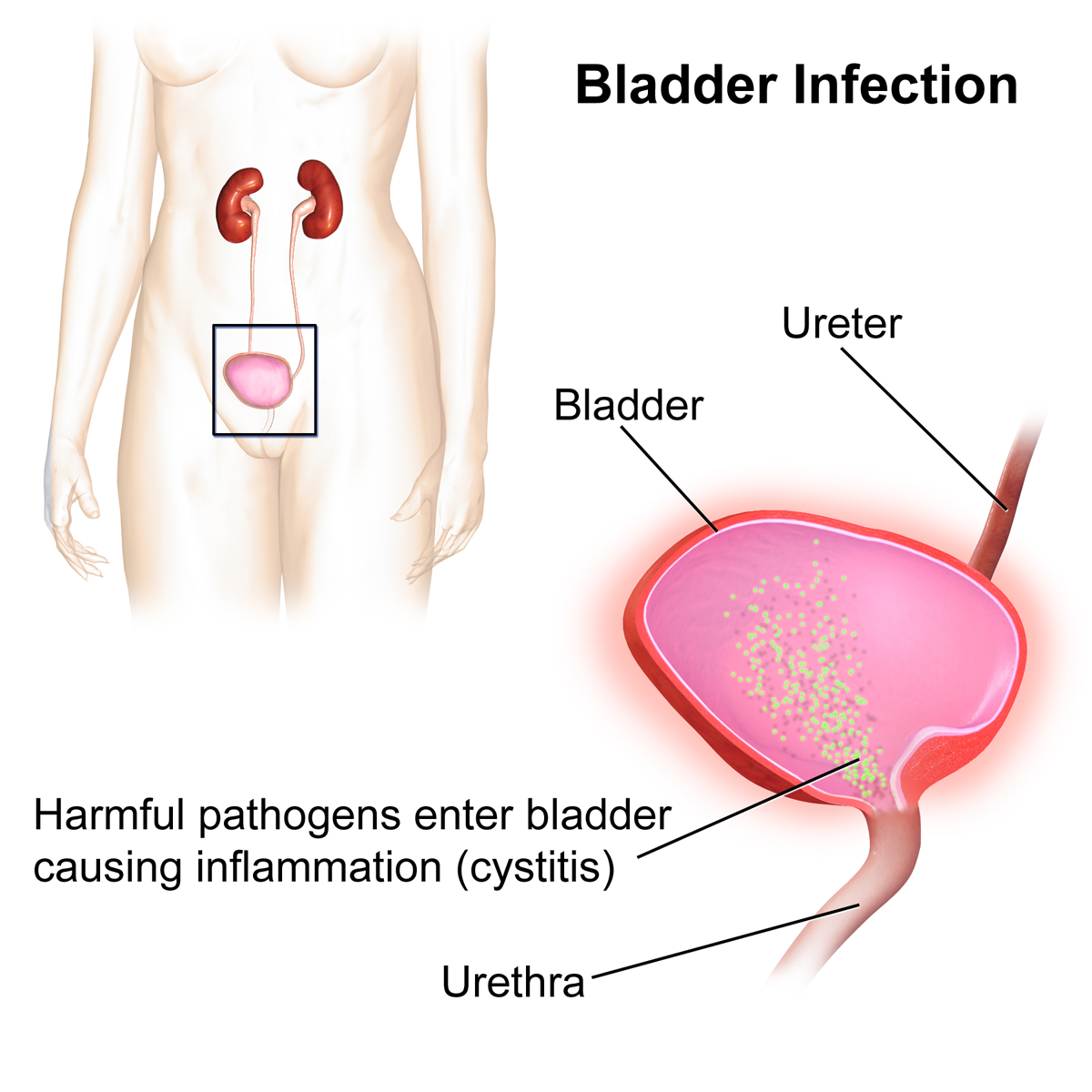
The bacteria that cause urinary tract infections typically enter the bladder via the urethra. However, infection may also occur via the blood or lymph. It is believed that the bacteria are usually transmitted to the urethra from the bowel, with females at greater risk due to their anatomy. After gaining entry to the bladder, E. Coli are able to attach to the bladder wall and form a biofilm that resists the body's immune response.
About half of the recurrent infection have the same strain as the first infection. This implies that there is a reservoir of the pathogen somewhere in the body. Potential locations of these reservoirs are the gut or vaginal micriobiome, or even the bladder itself. Bacteria that cause UTIs have been found in all three locations.
Diagnosis

In straightforward cases, a diagnosis may be made and treatment given based on symptoms alone without further laboratory confirmation.
Urine analysis
In complicated or questionable cases, it may be useful to confirm the diagnosis via urinalysis. For instance, a nitrate test can diagnose some UTIs, as a subset of bacteria produce this. Not all bacteria do however, so a negative test does not exclude a UTI. Other dipstick values useful for diagnosing UTIs are high pH (some bacteria split urea), the presence of blood and or leukocyte esterase. Another test, urine microscopy, looks for the presence of red blood cells, white blood cells, or bacteria.
Urine culture is deemed positive if it shows a bacterial colony count of greater than or equal to 103 colony-forming units per mL of a typical urinary tract organism. Antibiotic sensitivity can also be tested with these cultures, making them useful in the selection of antibiotic treatment. As symptoms can be vague and without reliable tests for urinary tract infections, diagnosis can be difficult in the elderly.
Classification
A urinary tract infection may involve only the lower urinary tract, in which case it is known as a bladder infection. Alternatively, it may involve the upper urinary tract, in which case it is known as pyelonephritis.
Children
To make the diagnosis of a urinary tract infection in children, a positive urinary culture is required. Contamination poses a frequent challenge depending on the method of collection used, thus a cutoff of 105CFU/mL is used for a "clean-catch" mid stream sample, 104CFU/mL is used for catheter-obtained specimens, and 102CFU/mL is used for suprapubic aspirations (a sample drawn directly from the bladder with a needle). The use of "urine bags" to collect samples is discouraged by the World Health Organization due to the high rate of contamination when cultured, and catheterization is preferred in those not toilet trained.
Some, such as the American Academy of Pediatrics recommends renal ultrasound and voiding cystourethrogram (watching a person's urethra and urinary bladder with real time x-rays while they urinate) in all children less than two years old who have had a urinary tract infection. However, because there is a lack of effective treatment if problems are found, others such as the National Institute for Health and Care Excellence only recommends routine imaging in those less than six months old or who have unusual findings.
Differential diagnosis
In women with cervicitis (inflammation of the cervix) or vaginitis (inflammation of the vagina) and in young men with UTI symptoms, a Chlamydia trachomatis or Neisseria gonorrhoeae infection may be the cause. These infections are typically classified as a urethritis rather than a urinary tract infection. Vaginitis may also be due to a yeast infection. Interstitial cystitis (chronic pain in the bladder) may be considered for people who experience multiple episodes of UTI symptoms but urine cultures remain negative and not improved with antibiotics. Prostatitis (inflammation of the prostate) may also be considered in the differential diagnosis.
Hemorrhagic cystitis, characterized by blood in the urine, can occur secondary to a number of causes including: infections, radiation therapy, underlying cancer, medications and toxins. Eosinophilic cystitis is a rare condition where eosinophiles are present in the bladder wall. Its cause is not entirely clear; however, it may be linked to food allergies, infections, and medications among others.
Prevention
A number of behaviors are recommended to prevent UTIs from recurring. They include urinating after sex, avoiding douching, wiping from front to back after defecation, and wearing breathable underwear. It is unclear how much these help; clinical guidelines typically regard the evidence as weak. NICE also recommends not holding up urine frequently and drinking sufficiently. There is lack of evidence surrounding the effect of tampon use. In those with frequent urinary tract infections who use spermicide or a diaphragm as a method of contraception, they are advised to use alternative methods.
Using urinary catheters as little and as short of time as possible and appropriate care of the catheter when used prevents catheter-associated urinary tract infections. They should be inserted using sterile technique in hospital however non-sterile technique may be appropriate in those who self catheterize. The urinary catheter set up should also be kept sealed.
Medications
For peri-menopausal or postmenopausal women with recurrent infections, topical vaginal estrogen has been found to reduce recurrence. For other people, or if topical estrogen does not work sufficiently, a single dose of antibiotics after a triggering event (like intercourse) can be considered. Methenamine is another medication used for prevention. As an anti-septic, antibiotic resistance does not develop against it.
European guidelines, including the UK guidelines, recommend a prolonged course of daily antibiotics after other options are proven ineffective or inappropriate. Where possible, the choice of antibiotic should be informed by a recent culture and the results of a susceptibility test. The American Urological Association recommends continuous antibiotics as one of many first-line options for recurrent UTIs.
Antibiotics following short term urinary catheterization decreases the subsequent risk of a bladder infection. A number of UTI vaccines are in development as of 2025.
Children
Low-dose antibiotics slightly reduces the risk of recurrent UTIs in children. However, the benefit is small, many children stop having repeat infections without antibiotics, and antibiotic use can increase the likelihood that future UTIs will be resistant to treatment. Circumcision of boys has been observed to exhibit a strong protective effect against UTIs, with some research suggesting as much as a 90% reduction in symptomatic UTI incidence among male infants, if they are circumcised. The protective effect is even stronger in boys born with urogenital abnormalities.
Dietary supplements
Cranberry products can reduce the risk of UTIs in certain groups (women with reoccurring UTIs, children, and people having had clinical interventions), but not in pregnant women, the elderly or people with urination disorders. They can also be used as an adjuvant to antibiotics and other standard treatments. Some evidence suggests that cranberry juice is more effective at UTI control than dehydrated tablets or capsules. Cranberry supplements are high in sugar content, which may worsen the risks associated with UTIs in patients with diabetes mellitus.
D-mannose is often marketed as a dietary supplement that prevents UTIs; however, there is little evidence supporting its use. A randomised controlled trial compared daily d-mannose with a placebo (fructose) among women with recurrent urinary tract infections over 6 months. D-mannose offered no benefit over placebo in reducing UTIs.
Certain probiotics might help reduce UTI recurrence, but evidence is weaker than for cranberries.
Treatment
The mainstay of treatment is antibiotics. Fosfomycin can be used as an effective treatment for both UTIs and complicated UTIs including acute pyelonephritis. The standard regimen for complicated UTIs is an oral 3 g dose administered once every 48 or 72 hours for a total of 3 doses or a 6 grams every 8 hours for 7 days to 14 days when fosfomycin is given in IV form. Gepotidacin was approved for medical use in the United States in March 2025. It is the first new antibiotic approved in the US for UTIs in nearly 30 years.
Phenazopyridine is occasionally prescribed during the first few days in addition to antibiotics to help with the burning and urgency sometimes felt during a bladder infection. However, it is not routinely recommended due to safety concerns with its use, specifically an elevated risk of methemoglobinemia (higher than normal level of methemoglobin in the blood). Paracetamol may be used for fevers. There is no good evidence for the use of cranberry products for treating current infections.
Uncomplicated
Uncomplicated infections can be diagnosed and treated based on symptoms alone. Antibiotics taken by mouth such as nitrofurantoin, pivmecillinam, or fosfomycin are typically first line. Fosfomycin may be used as a single dose, whereas nitrofurantoin and pivmecillinam require a 3 to 5 day course. Cephalosporins, amoxicillin/clavulanic acid, or a fluoroquinolone may also be used. Antibiotic resistance to bacteria that cause UTIs has been increasing, and trimethoprim/sulfamethoxazole is now only recommended in areas with low E. coli antibiotic resistance.
The Food and Drug Administration (FDA) recommends against the use of fluoroquinolones, including a Boxed Warning, when other options are available due to higher risks of serious side effects, such as tendinitis, tendon rupture and worsening of myasthenia gravis. The Infectious Diseases Society of America noted concern of generating resistance to this class of medication. Amoxicillin-clavulanate appears less effective than other options. For simple UTIs, children often respond to a three-day course of antibiotics. The combination sulopenem etzadroxil/probenecid (Orlynvah) was approved for medical use in the United States in October 2024.
Women with recurrent simple UTIs are over 90% accurate in identifying new infections. They may benefit from self-treatment upon occurrence of symptoms with medical follow-up only if the initial treatment fails.
For mild to moderate uncomplicated UTIs, antibiotics may be completely avoided initially, following discussion with the patient. For instance, ibuprofen can be recommended while a culture is performed to confirm diagnosis and to test how susceptible the infection is to various antibiotics. Delaying or avoiding antibiotics leads to a longer recovery period, but many UTIs do resolve without antibiotics. The risk of progression to a kidney infection is higher than with antibiotic use, but remains low. A 'wait-and-see' antibiotic prescription can be provided. Overall, this strategy substantially reduces antibiotic use.
Complicated
Complicated UTIs are more difficult to treat and usually requires more aggressive evaluation, treatment, and follow-up. It may require identifying and addressing the underlying complication. Increasing antibiotic resistance is causing concern about the future of treating those with complicated and recurrent UTI.
Asymptomatic bacteriuria
Those who have bacteria in the urine but no symptoms should not generally be treated with antibiotics. This includes those who are old, those with spinal cord injuries, and those who have urinary catheters. Pregnancy is an exception and it is recommended that women take sevendays of antibiotics. If not treated it causes up to 30% of mothers to develop pyelonephritis and increases risk of low birth weight and preterm birth. Some also support treatment of those with diabetes mellitus and treatment before urinary tract procedures which will likely cause bleeding.
Pregnant women
Urinary tract infections, even asymptomatic presence of bacteria in the urine, are more concerning in pregnancy due to the increased risk of kidney infections. During pregnancy, high progesterone levels elevate the risk of decreased muscle tone of the ureters and bladder, which leads to a greater likelihood of reflux, where urine flows back up the ureters and towards the kidneys. While pregnant women do not have an increased risk of asymptomatic bacteriuria, if bacteriuria is present they do have a 25–40% risk of a kidney infection. Thus if urine testing shows signs of an infection—even in the absence of symptoms—treatment is recommended. Cephalexin or nitrofurantoin are typically used because they are generally considered safe in pregnancy. A kidney infection during pregnancy may result in preterm birth or pre-eclampsia (a state of high blood pressure and kidney dysfunction during pregnancy that can lead to seizures). Some women have UTIs that keep coming back in pregnancy. There is insufficient research on how to best treat these recurrent infections.
Pyelonephritis
Pyelonephritis is treated more aggressively than a simple bladder infection using either a longer course of oral antibiotics or intravenous antibiotics. In those who exhibit more severe symptoms, admission to a hospital for ongoing antibiotics may be needed. Complications such as ureteral obstruction from a kidney stone may be considered if symptoms do not improve following two or three days of treatment.
Prognosis
With treatment, symptoms generally improve within 36hours.
15–25% of adults and children have chronic symptomatic UTIs including recurrent infections, persistent infections (infection with the same pathogen), a re-infection (new pathogen), or a relapsed infection (the same pathogen causes a new infection after it was completely gone). Recurrent urinary tract infections are defined as at least two infections (episodes) in a six-month time period or three infections in twelve months, can occur in adults and in children.
About 10–20% of children of upper urinary tract infection which involves the kidney (pyelonephritis) will go on and develop scarring of the affected kidney. Then, 10–20% of those develop scarring will have increased risk of hypertension in later life. Recurrent UTIs are a rare cause of further kidney problems if there are no underlying abnormalities of the kidneys, resulting in less than a third of a percent (0.33%) of chronic kidney disease in adults.
Epidemiology
Urinary tract infections occur almost four times more frequently in females than males. Urinary tract infections are the most frequent bacterial infection in women. They occur most frequently between the ages of 16 and 35years, with 10% of women getting an infection yearly and more than 40–60% having an infection at some point in their lives. Recurrences are common, with nearly half of people getting a second infection within a year.
Pyelonephritis occurs between 20 and 30 times less frequently. Rates of asymptomatic bacteria in the urine increase with age from two to seven percent in women of child-bearing age to as high as 50% in elderly women in care homes.
Urinary tract infections may affect 10% of people during childhood. Among children, urinary tract infections are most common in uncircumcised males less than three months of age, followed by females less than one year. Estimates of frequency among children, however, vary widely. In a group of children with a fever, ranging in age between birth and two years, 2–20% were diagnosed with a UTI.
Veterinary medicine
Domestic cats are less susceptible to bacterial urinary tract infections than domestic dogs.
History
Urinary tract infections have been described since ancient times with the first documented description in the Ebers Papyrus dated to c. 1550 BC. Effective treatment did not occur until the development and availability of antibiotics in the 1930s, before which time herbs, bloodletting and rest were recommended.
References
References
- (May 2015). "Urinary tract infections: epidemiology, mechanisms of infection and treatment options". Nature Reviews. Microbiology.
- (2003). "In a Page: Emergency medicine". Lippincott Williams & Wilkins.
- (2025-02-08). "Epidemiological trends and predictions of urinary tract infections in the global burden of disease study 2021". Scientific Reports.
- CDC. (2024-04-24). "Urinary Tract Infection Basics".
- (August 2011). "Diagnosis and management of urinary tract infection and pyelonephritis". Emergency Medicine Clinics of North America.
- (17 April 2015). "Urinary Tract Infection".
- (February 2011). "Diagnosis and management of urinary infections in older people". Clinical Medicine.
- (2025). "Urinary tract infections (UTIs)".
- (2015). "Introduction to Medical-Surgical Nursing". Elsevier Health Sciences.
- (February 2008). "Uncomplicated urinary tract infection in adults including uncomplicated pyelonephritis". The Urologic Clinics of North America.
- (2007). "Bennett & Brachman's hospital infections.". Wolters Kluwer Health/Lippincott Williams & Wilkins.
- (September 2011). "Diagnosis and treatment of acute pyelonephritis in women". American Family Physician.
- (November 2015). "Asymptomatic Bacteriuria in Noncatheterized Adults". The Urologic Clinics of North America.
- (2024). "European Association of Urology Guidelines on Urological Infections: Summary of the 2024 Guidelines". European Urology.
- (October 2011). "Diagnosis and treatment of acute uncomplicated cystitis". American Family Physician.
- (June 2011). "Urinary tract infections in women". European Journal of Obstetrics, Gynecology, and Reproductive Biology.
- (2008). "An introduction to botanical medicines: history, science, uses, and dangers". Praeger Publishers.
- (19 January 2011). "Non-vascular interventional radiology of the abdomen". Springer.
- (September 2019). "Risk of Meningitis in Infants Aged 29 to 90 Days with Urinary Tract Infection: A Systematic Review and Meta-Analysis". The Journal of Pediatrics.
- (2021). "Associations of delirium with urinary tract infections and asymptomatic bacteriuria in adults aged 65 and older: A systematic review and meta-analysis". Journal of the American Geriatrics Society.
- (2025). "Purple urine bag syndrome: An unusual presentation of urinary tract infection: A case series and literature review". Medicine.
- (February 2014). "Ten Things Physicians and Patients Should Question". AMDA – The Society for Post-Acute and Long-Term Care Medicine.
- (2025). "Urinary tract infections: pathogenesis, host susceptibility and emerging therapeutics". Nature Reviews Microbiology.
- (November 2011). "Probiotic therapy: immunomodulating approach toward urinary tract infection". Current Microbiology.
- "Urinary Tract Infections in Adults".
- (April 2010). "Diagnosis and treatment of urethritis in men". American Family Physician.
- (15 July 2008). "Redefining Urological History Taking – Anal Intercourse as the Cause of Unexplained Symptoms in Heterosexuals". The Annals of the Royal College of Surgeons of England.
- Dunkin, Mary. (2024-04-11). "Anal Sex Safety: What to Know".
- (2013). "Study Guide for Pathophysiology". Elsevier Health Sciences.
- (January 2011). "Urinary tract infections in women". The Medical Clinics of North America.
- (December 2013). "Multidisciplinary overview of vaginal atrophy and associated genitourinary symptoms in postmenopausal women". Sexual Medicine.
- (February 2016). "Common Questions About Chronic Prostatitis". American Family Physician.
- (December 2009). "Genitourinary infection and barotrauma as complications of 'P-valve' use in drysuit divers". Diving and Hyperbaric Medicine.
- (June 2013). "Circumcision and lifetime risk of urinary tract infection: a systematic review and meta-analysis". The Journal of Urology.
- (April 2010). "Prevention of urinary tract infections in persons with spinal cord injury in home health care". Home Healthcare Nurse.
- (2025). "Uncomplicated Urinary Tract Infection". Statpearls.
- (August 2011). "Pediatric urinary tract infections". Emergency Medicine Clinics of North America.
- (15 January 2011). "Approach to internal medicine: a resource book for clinical practice". Springer.
- (2000). "Office urology". Humana Press.
- (2006). "Blueprints emergency medicine". Lippincott Williams & Wilkins.
- (2009). "Glenn's urologic surgery". Lippincott Williams & Wilkins.
- (2002). "Clinical pediatric urology". Dunitz.
- (February 2009). "The spectrum of eosinophilic cystitis in males: case series and literature review". Archives of Pathology & Laboratory Medicine.
- (2022). "Guideline of guidelines: management of recurrent urinary tract infections in women". BJU International.
- (February 2025). "Scenario: Recurrent UTI (no haematuria, not pregnant or catheterised)".
- (May 2001). "The chronic indwelling catheter and urinary infection in long-term-care facility residents". Infection Control and Hospital Epidemiology.
- (April 2010). "Guideline for prevention of catheter-associated urinary tract infections 2009". Infection Control and Hospital Epidemiology.
- (September 2014). "Types of indwelling urethral catheters for short-term catheterisation in hospitalised adults". The Cochrane Database of Systematic Reviews.
- (April 2016). "Non-Antibiotic Prophylaxis for Urinary Tract Infections". Pathogens.
- NICE. (2024). "Recommendations {{!}} Urinary tract infection (recurrent): antimicrobial prescribing {{!}} Guidance".
- "Recurrent Uncomplicated Urinary Tract Infections in Women: AUA/CUA/SUFU Guideline (2025) - American Urological Association".
- (June 2013). "Antibiotic prophylaxis for urinary tract infections after removal of urinary catheter: meta-analysis". BMJ.
- (2019-04-01). "Long-term antibiotics for preventing recurrent urinary tract infection in children". Cochrane Database of Systematic Reviews.
- (Apr 2008). "Prevalence of Urinary Tract Infection in Childhood: A Meta-Analysis". Pediatric Infectious Disease Journal.
- (Feb 2018). "Canadian Urological Association guideline on the care of the normal foreskin and neonatal circumcision in Canadian infants (full version)". Canadian Urological Association Journal.
- (November 2023). "Cranberries for preventing urinary tract infections". The Cochrane Database of Systematic Reviews.
- (2 September 2021). "Consumption of cranberry as adjuvant therapy for urinary tract infections in susceptible populations: A systematic review and meta-analysis with trial sequential analysis". PLOS ONE.
- (17 October 2012). "Cranberries for preventing urinary tract infections". The Cochrane Database of Systematic Reviews.
- (1 June 2024). "d-Mannose for Prevention of Recurrent Urinary Tract Infection Among Women: A Randomized Clinical Trial". JAMA Internal Medicine.
- (6 February 2025). "D-mannose does not prevent urinary tract infections". NIHR Evidence.
- (2024). "Update of the Spanish clinical practice guideline for urinary tract infection in infants and children. Summary of recommendations for diagnosis, treatment and follow-up". Anales de Pediatría (English Edition).
- (28 March 2020). "Oral and Intravenous Fosfomycin for the Treatment of Complicated Urinary Tract Infections". Hindawi Limited.
- (25 March 2025). "Blujepa (gepotidacin) approved by US FDA for treatment of uncomplicated urinary tract infections (uUTIs) in female adults and pediatric patients 12 years of age and older".
- (25 March 2025). "FDA approves first new antibiotic for UTIs in nearly 30 years".
- Goodman, Brenda. (25 March 2025). "Millions of women get painful UTIs that keep coming back. A new kind of antibiotic may help break the cycle".
- (June 2004). "Phenazopyridine hydrochloride: the use and abuse of an old standby for UTI". Urologic Nursing.
- (2008). "Meyler's side effects of analgesics and anti-inflammatory drugs". Elsevier Science.
- (2010). "Family practice guidelines". Springer.
- (January 2007). "Cranberry juice for the prevention and treatment of urinary tract infections". Drugs of Today.
- (2009). "Cranberry and urinary tract infections". Drugs.
- (8 March 2018). "FDA Drug Safety Communication: FDA updates warnings for oral and injectable fluoroquinolone antibiotics due to disabling side effects".
- (March 2011). "International clinical practice guidelines for the treatment of acute uncomplicated cystitis and pyelonephritis in women: A 2010 update by the Infectious Diseases Society of America and the European Society for Microbiology and Infectious Diseases". Clinical Infectious Diseases.
- (December 2012). "Comparative effectiveness of antibiotics for uncomplicated urinary tract infections: network meta-analysis of randomized trials". Family Practice.
- (15 December 2006). "BestBets: Is a short course of antibiotics better than a long course in the treatment of UTI in children".
- (1 October 2024). "FDA approves new treatment for women with uncomplicated UTIs".
- (25 October 2024). "Iterum Therapeutics Receives U.S. FDA Approval of Orlynvah (Oral Sulopenem) for the Treatment of Uncomplicated Urinary Tract Infections".
- (2023-12-02). "Treating urinary tract infections in the era of antibiotic resistance". Expert Review of Anti-infective Therapy.
- (2002). "Infectious diseases in primary care". W.B. Saunders.
- (March 2013). "Prevention of recurrent urinary tract infections". Minerva Urologica e Nefrologica.
- (November 2010). "Complicated urinary tract infections: practical solutions for the treatment of multiresistant Gram-negative bacteria". The Journal of Antimicrobial Chemotherapy.
- (July 2013). "Management of urinary tract infections in the era of increasing antimicrobial resistance". The Medical Clinics of North America.
- (November 2018). "Ceftriaxone treatment of complicated urinary tract infections as a risk factor for enterococcal re-infection and prolonged hospitalization: A 6-year retrospective study". Bosnian Journal of Basic Medical Sciences.
- (October 2011). "Asymptomatic bacteriuria - prevalence in the elderly population". Australian Family Physician.
- (September 2006). "Asymptomatic bacteriuria in adults". American Family Physician.
- "Five Things Physicians and Patients Should Question". American Geriatrics Society.
- (November 2015). "Duration of treatment for asymptomatic bacteriuria during pregnancy". The Cochrane Database of Systematic Reviews.
- (September 2010). "Different antibiotic regimens for treating asymptomatic bacteriuria in pregnancy". The Cochrane Database of Systematic Reviews.
- (October 2013). "Genitourinary infection in diabetes". Indian Journal of Endocrinology and Metabolism.
- (July 2015). "Interventions for preventing recurrent urinary tract infection during pregnancy". The Cochrane Database of Systematic Reviews.
- (2011). "The Sanford Guide to Antimicrobial Therapy 2011 (Guide to Antimicrobial Therapy (Sanford))". Antimicrobial Therapy.
- (November 2018). "The Emergency Department Diagnosis and Management of Urinary Tract Infection". Emergency Medicine Clinics of North America.
- (August 2022). "D-mannose for preventing and treating urinary tract infections". The Cochrane Database of Systematic Reviews.
- (March 1996). "A review of renal scarring in children". Nuclear Medicine Communications.
- (November 2011). "Childhood urinary tract infections as a cause of chronic kidney disease". Pediatrics.
- (1 November 2019). "Urinary tract infection and subclinical bacteriuria in cats: A clinical update". Journal of Feline Medicine and Surgery.
- (1990). "Topley and Wilson's Principles of bacteriology, virology and immunity: in 4 volumes". Arnold.
This article was imported from Wikipedia and is available under the Creative Commons Attribution-ShareAlike 4.0 License. Content has been adapted to SurfDoc format. Original contributors can be found on the article history page.
Ask Mako anything about Urinary tract infection — get instant answers, deeper analysis, and related topics.
Research with MakoFree with your Surf account
Create a free account to save articles, ask Mako questions, and organize your research.
Sign up freeThis content may have been generated or modified by AI. CloudSurf Software LLC is not responsible for the accuracy, completeness, or reliability of AI-generated content. Always verify important information from primary sources.
Report