From Surf Wiki (app.surf) — the open knowledge base
Reduction (orthopedic procedure)
Surgery to repair fractures or dislocations
Surgery to repair fractures or dislocations

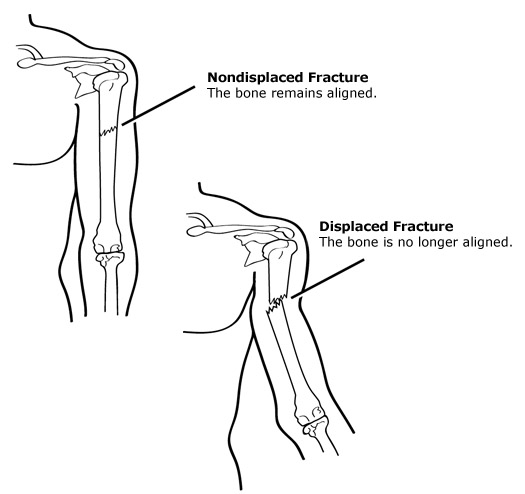
Reduction is a medical procedure to restore the correct anatomical alignment of a fracture or dislocation. When an injury results in a fracture, or broken bone, the bone segments can sometimes become misaligned. This is referred to as a displaced fracture, which requires the medical procedure called reduction. Some providers may refer to this as 'setting the bone'. When an injury results in a dislocation of a joint, or the misalignment of two connecting bones, a similar process of reduction must be performed to relocate the joint back into normal anatomical positioning. In the case of both displaced fractures and joint dislocation reduction is required for effective healing.
Fracture reduction
There are two main categories of fracture reductions: closed reductions and open reductions. Both procedures require confirmatory imaging – such as X-ray – both before the reduction to confirm the misalignment of bones and after the reduction procedure to confirm successful achievement of anatomical positioning.
Closed reduction
Closed reduction is when bone alignment is achieved from external manipulation of the bone without having to open the skin. This is not a surgical procedure and is often performed in the emergency department with local anesthetic for pain management. A distal radial fracture (wrist) is a common injury that requires a closed reduction.
Open reduction
Open reduction is a surgical procedure in which bone alignment is achieved from internal manipulation of the bone when the skin is open. After reduction of the fractured site, it is common that fixed hardware is put in place to maintain anatomical alignment during bone healing; this process is called fixation. While many open reductions require either internal (ORIF) or external fixation (OREF) there are some fractures that, after open reduction, do not require fixation.

Dislocation reduction
Reductions for dislocations are dependent on the joint they involve. Common dislocations include the shoulder, finger, hip, knee and patella. In children, the elbow is also a common dislocation and referred to as nursemaid's elbow. There are many techniques but the same tenets are generally applied to all dislocation reductions. Traction, or sustained pulling pressure, is applied to the distal bone of the dislocated joint to relax the surrounding musculature and create space for the bone to move back into anatomical position. Traction can be applied either by human strength or with a system of pulleys and weights. Surrounding muscles, nerves and vasculature can be disrupted during the initial injury which can result in further surgical requirements even if proper bone alignment is achieved.
Procedural medications
Open reductions are done under general anesthesia administered by anesthesiologists in the operating room. Closed reductions are most often done with the aid of multimodal pain medications, sedatives and/or local anesthesia. Commonly a state of moderate sedation, or conscious sedation, is desired to reduce patient stress from the experience and relax the patient to improve in the manipulation during reduction. Ketamine and Midazolam are common choices for pediatric conscious sedations and are often given in conjunction with a short acting opiate like fentanyl. In adults, propofol, midazolam and etomidate are frequently used for conscious sedation with a short acting opiate like fentanyl. Local hematoma blocks are also commonly employed for the reduction of forearm fractures. Hematoma blocks are when a local anesthetic like lidocaine is injected into the fracture site under the guidance of ultrasound to allow for fracture manipulation and reduction without pain or the need for systemic medications. NSAIDs and acetaminophen continue to be mainstays of pain management due to their efficacy and safety.
Procedural risks and complications
Risks and complications from reductions include but are not limited to further damage to the fracture or dislocation, and damage to surrounding structures and tissues such as nerves, muscles, and blood vessels. There is also a risk of an unsuccessful reduction, which might require multiple attempts and prolonged need for medication administration or switching to a surgical intervention, in the case of dislocations and closed fractures. The medications administered during the procedure such as medications to block pain (local or general anesthetic) also have side effect profiles and risks of administration. Open reductions carry the risks of any orthopedic surgery, including but not limited to infection, hardware failures, damage to surrounding structures, and adverse reactions to general anesthesia.
TOC
Recovery and rehabilitation
After a closed reduction, pain is expected for 2–3 weeks and potentially milder pain for up to 6 weeks.
References
- (primary source)
References
- (2025-02-06). "General Principles of Fracture Care Treatment & Management: Approach Considerations, Elements of Initial Fracture Management, Nonoperative Therapy". Medscape.
- "Dislocation: MedlinePlus Medical Encyclopedia".
- "Closed reduction of a fractured bone: MedlinePlus Medical Encyclopedia".
- (2006-01-01). "Sedation and Analgesia for Pediatric Fracture Reduction in the Emergency Department: A Systematic Review". Archives of Pediatrics & Adolescent Medicine.
- (February 2013). "Sedation-assisted Orthopedic Reduction in Emergency Medicine: The Safety and Success of a One Physician/One Nurse Model". The Western Journal of Emergency Medicine.
- Blakeney, William G.. (2010-11-18). "Stabilization and treatment of Colles' fractures in elderly patients". Clinical Interventions in Aging.
- "Bone fracture repair - series—Procedure: MedlinePlus Medical Encyclopedia".
- (May 1998). "Open reduction without fixation of dislocated condylar process fractures: long-term clinical and radiologic analysis". Journal of Oral and Maxillofacial Surgery.
- (1992). "Treatment of mandibular fractures with or without intermaxillary fixation--a comparative study". Oral Surgery, Oral Diagnosis.
- (February 1999). "Intermaxillary fixation is not usually necessary to reduce mandibular fractures". British Journal of Oral and Maxillofacial Surgery.
- "Traction: MedlinePlus Medical Encyclopedia".
- (2025). "Shoulder Dislocations Overview". StatPearls Publishing.
- "Statement on Continuum of Depth of Sedation: Definition of General Anesthesia and Levels of Sedation/Analgesia".
- (2000-03-30). "Sedation and Analgesia for Procedures in Children". New England Journal of Medicine.
- (October 1998). "Comparison of fentanyl/midazolam with ketamine/midazolam for pediatric orthopedic emergencies". Pediatrics.
- (2018-10-01). "Intra-articular Hematoma Block Compared to Procedural Sedation for Closed Reduction of Ankle Fractures". Foot & Ankle International.
- (2015-03-01). "Ultrasound-guided Hematoma Block for Distal Radial and Ulnar Fractures". The Journal of Emergency Medicine.
- Slawson, David. (2018-03-01). "Ibuprofen Plus Acetaminophen Equals Opioid Plus Acetaminophen for Acute Severe Extremity Pain". American Family Physician.
- "Closed Reduction of a Fractured Bone: What to Expect at Home".
This article was imported from Wikipedia and is available under the Creative Commons Attribution-ShareAlike 4.0 License. Content has been adapted to SurfDoc format. Original contributors can be found on the article history page.
Ask Mako anything about Reduction (orthopedic procedure) — get instant answers, deeper analysis, and related topics.
Research with MakoFree with your Surf account
Create a free account to save articles, ask Mako questions, and organize your research.
Sign up freeThis content may have been generated or modified by AI. CloudSurf Software LLC is not responsible for the accuracy, completeness, or reliability of AI-generated content. Always verify important information from primary sources.
Report