From Surf Wiki (app.surf) — the open knowledge base
Pertussis vaccine
Vaccine protecting against whooping cough
Vaccine protecting against whooping cough
| Field | Value |
|---|---|
| Verifiedfields | changed |
| verifiedrevid | 402053071 |
| type | vaccine |
| image | DPT-IPV-japan Quattro back.jpg |
| caption | Pertussis vaccination is often administered via a combined DPT vaccine or, as shown here, a DTaP-IPV vaccine |
| target | Whooping cough |
| vaccine_type | Inactivated, subunit |
| MedlinePlus | a682198 |
| DailyMedID | Pertussis vaccine |
| pregnancy_AU | |
| ATC_prefix | J07 |
| ATC_suffix | AJ01 |
| ATC_supplemental | |
| legal_AU | |
| legal_BR | |
| legal_CA | |
| legal_DE | |
| legal_NZ | |
| legal_UK | |
| legal_US | Rx-only |
| legal_UN | |
| legal_status | Rx-only |
| CAS_number_Ref | |
| DrugBank_Ref | |
| DrugBank | DB15274 |
| ChemSpiderID_Ref | |
| ChemSpiderID | none |
| UNII | 2QNL82089R |
| Drugs.com =
Pertussis vaccine is a vaccine that protects against whooping cough (pertussis). There are two main types: whole-cell vaccines and acellular vaccines. The effectiveness of the vaccines appears to decrease by between 2 and 10% per year after vaccination, with a more rapid decrease with the acellular vaccines.
Vaccinating the mother during pregnancy may protect the baby. Three doses starting at six weeks of age are typically recommended in young children. Additional doses may be given to older children and adults. This recommendation includes people who have HIV/AIDS.
The acellular vaccines are more commonly used in the developed world due to fewer adverse effects. Between 10 and 50% of people given the whole-cell vaccines develop redness at the injection site or fever. Febrile seizures and long periods of crying occur in less than 1% of people. With the acellular vaccines a brief period of non-serious swelling of the arm may occur. Side effects with both types of vaccines, but especially the whole-cell vaccine, are less common the younger the child. The whole-cell vaccines should not be used after seven years of age. Serious long-term neurological problems are not associated with either type.
The pertussis vaccine was developed in 1926. It is on the World Health Organization's List of Essential Medicines.
Medical uses
Effectiveness
Acellular pertussis vaccine (aP) with three or more antigens prevents around 85% of typical whooping cough cases in children. Compared to the whole cell pertussis vaccine (wP) used previously, the efficacy of aP declines faster. Multi-antigen aP has higher efficacy than old low-efficacy wP, but is possibly less effective than the highest-efficacy wP vaccines. Acellular vaccines also cause fewer side effects than whole-cell vaccines.
Despite widespread vaccination, pertussis has persisted in vaccinated populations and is one of the most common vaccine-preventable diseases. The recent resurgence in pertussis infections is attributed to a combination of waning immunity and new mutations in the pathogen that existing vaccines are unable to effectively control. It is debated whether the switch from wP to aP has played a role in this resurgence, with two 2019 articles disagreeing with one another.
Some studies have suggested that while acellular pertussis vaccines are effective at preventing the disease, they have a limited impact on infection and transmission, meaning that vaccinated people could spread the disease even though they may have only mild symptoms or none at all.
Children
For children, immunizations are commonly given in combination with immunizations against tetanus, diphtheria, polio, and haemophilus influenzae type B at two, four, six, and 15–18 months of age.
Adults
In 2006, the US Centers for Disease Control and Prevention (CDC) recommended adults receive pertussis vaccination along with the tetanus and diphtheria toxoid booster. The UK commenced routine vaccination of pregnant women in 2012. The program initially aimed to vaccinate women between 28 and 32 weeks (but up to 38 weeks) of pregnancy: later advise allowed maternal pertussis immunisation from week 16 of pregnancy. Since its introduction the maternal pertussis immunisation programme is very effective in protecting infants until they can have their first vaccinations at two months of age. During the first year of the maternal immunization programme in Britain, the average vaccine coverage in England was 64% and vaccine effectiveness was estimated to be 91%. During 2012 fourteen infants died from pertussis in England and Wales; all were born before the introduction of the programme. Up to 31 October 2014, 10 deaths were reported in infants with confirmed whooping cough who were born after the introduction of the maternal programme. Nine of them were born to unvaccinated mothers and all 10 were too young to have received a dose of pertussis-containing vaccine.
The pertussis booster for adults is combined with a tetanus vaccine and diphtheria vaccine booster; this combination is abbreviated "Tdap" (Tetanus, diphtheria, acellular pertussis). It is similar to the childhood vaccine called "DTaP" (Diphtheria, Tetanus, acellular Pertussis), with the main difference that the adult version contains smaller amounts of diphtheria and pertussis components—this is indicated in the name by the use of lower-case "d" and "p" for the adult vaccine. The lower-case "a" in each vaccine indicates that the pertussis component is acellular, or cell-free, which reduces the incidence of side effects. The pertussis component of the original DPT vaccine accounted for most of the minor local and systemic side effects in many vaccinated infants (such as mild fever or soreness at the injection site). The newer acellular vaccine, known as DTaP, has greatly reduced the incidence of adverse effects compared to the earlier "whole-cell" pertussis vaccine; however, immunity wanes faster after the acellular vaccine than the whole-cell vaccine.
Side effects
Between 10% and 50% of people given the whole-cell vaccines develop redness, swelling, soreness or tenderness at the injection site and/or fever, less than 1% experience febrile seizures or long periods of crying, and less than 1 out of every 1,000 to 2,000 people vaccinated have a hypotonic-hyporesponsive episode. Side effects with both types of vaccines, but especially the whole-cell vaccine, are more likely the older the child. The whole-cell vaccines should not be used after seven years of age. According to the WHO serious long-term neurological problems are not associated with either type. The WHO says that the only contraindication to either whole cell or acellular pertussis vaccines is an anaphylactic reaction to a previous dose of pertussis vaccine, while the US Centers for Disease Control and Prevention (CDC) lists encephalopathy not due to another identifiable cause occurring within seven days after a previous dose of pertussis vaccine as a contraindication and recommends those who have had seizures, have a known or suspected neurological disorder or have had a neurologic event after a previous dose not be vaccinated until after treatment is initiated and the condition stabilized. Only the acellular vaccine is used in the US.
Modern formulations
Whole-cell pertussis vaccines contain the entire inactivated organism while acellular pertussis vaccines contain parts (subunits) including the pertussis toxin alone or with components such as filamentous haemagglutinin, fimbrial antigens and pertactin. Whole-cell (wP) remains the vaccine of choice in low and middle-income countries, as it is cheaper and easier to produce.
, there are four acellular DTaP/Tdap vaccines licensed for use in the United States: Infanrix and Daptacel for children, Boostrix and Adacel for adolescents and adults. As of April 2016, the United Kingdom authorized five multivalent vaccines that include pertussis components: Pediacel, Infanrix-IPV+Hib, Repevax, Infanrix-IPV, and Boostrix-IPV.
| Vaccine | Producer | Licensed for | Pertussis toxin (PT), μg | Filamentous hemagglutinin (FHA), μg | Pertactin (PRN), μg | Fimbriae (FIM), μg |
|---|---|---|---|---|---|---|
| Infanrix | GlaxoSmithKline | 6 weeks through 6 years | 25 | 25 | 8 | – |
| Boostrix | GlaxoSmithKline | 10 years and older | 8 | 8 | 2.5 | – |
| Daptacel | Sanofi Pasteur | 6 weeks through 6 years | 10 | 5 | 3 | 5 |
| Adacel | Sanofi Pasteur | 10 through 64 years | 2.5 | 5 | 3 | 5 |
| Pediarix | GlaxoSmithKline | 6 weeks through 6 years | 10 | |||
| Kinrix | GlaxoSmithKline | |||||
| Quadracel | Sanofi Pasteur | |||||
| Vaxelis | MSP Vaccine Company | 6 weeks through 4 years | ||||
| Pentacel | Sanofi Pasteur | 6 weeks through 4 years | ||||
| Pediacel | Sanofi Pasteur | 6 weeks to 4 | 20 | 20 | 3 | 5 |
| Infanrix-IPV+Hib | GlaxoSmithKline | from 2 months | 25 | 25 | 8 | - |
| Repevax | Sanofi Pasteur | from 3 years | 2.5 | 5 | 3 | 5 |
| Infanrix-IPV | GlaxoSmithKline | 16 months to 13 years | 25 | 25 | 8 | - |
| Boostrix-IPV | GlaxoSmithKline | from 4 years | 8 | 8 | 2.5 | - |
History
Pearl Kendrick, Loney Gordon and Grace Eldering studied pertussis in the 1930s.
The pertussis vaccine is usually administered as a component of the diphtheria-tetanus-pertussis (DTP/DTwP, DTaP, and Tdap) vaccines. There are several types of diphtheria-tetanus-pertussis vaccines. The first vaccine against pertussis was developed in the 1930s by pediatrician Leila Denmark. It included whole-cell killed Bordetella pertussis bacteria. Until the beginning of the 1990s, it was used as a part of the DTwP vaccine for the immunization of children. It, however, contained pertussis endotoxin (surface lipooligosaccharide) and produced side effects.
New acellular pertussis vaccines were developed in the 1980s, which included only a few selected pertussis antigens (toxins and adhesins). They became a part of DTaP vaccines for children. These (Tdap) vaccines contain reduced amounts of pertussis antigens compared to DTaP vaccines.
Controversy in the 1970s–1980s
During the 1970s and 1980s, a controversy erupted related to the question of whether the whole-cell pertussis component caused permanent brain injury in rare cases, called pertussis vaccine encephalopathy. Despite this allegation, doctors recommended the vaccine due to the overwhelming public health benefit, because the claimed rate was very low (one case per 310,000 immunizations, or about 50 cases out of the 15 million immunizations each year in the United States), and the risk of death from the disease was high (pertussis killed thousands of Americans each year before the vaccine was introduced). No studies showed a causal connection, and later studies showed no connection of any type between the DPT vaccine and permanent brain injury. The alleged vaccine-induced brain damage proved to be an unrelated condition, infantile epilepsy. In 1990, the Journal of the American Medical Association called the connection a "myth" and "nonsense".
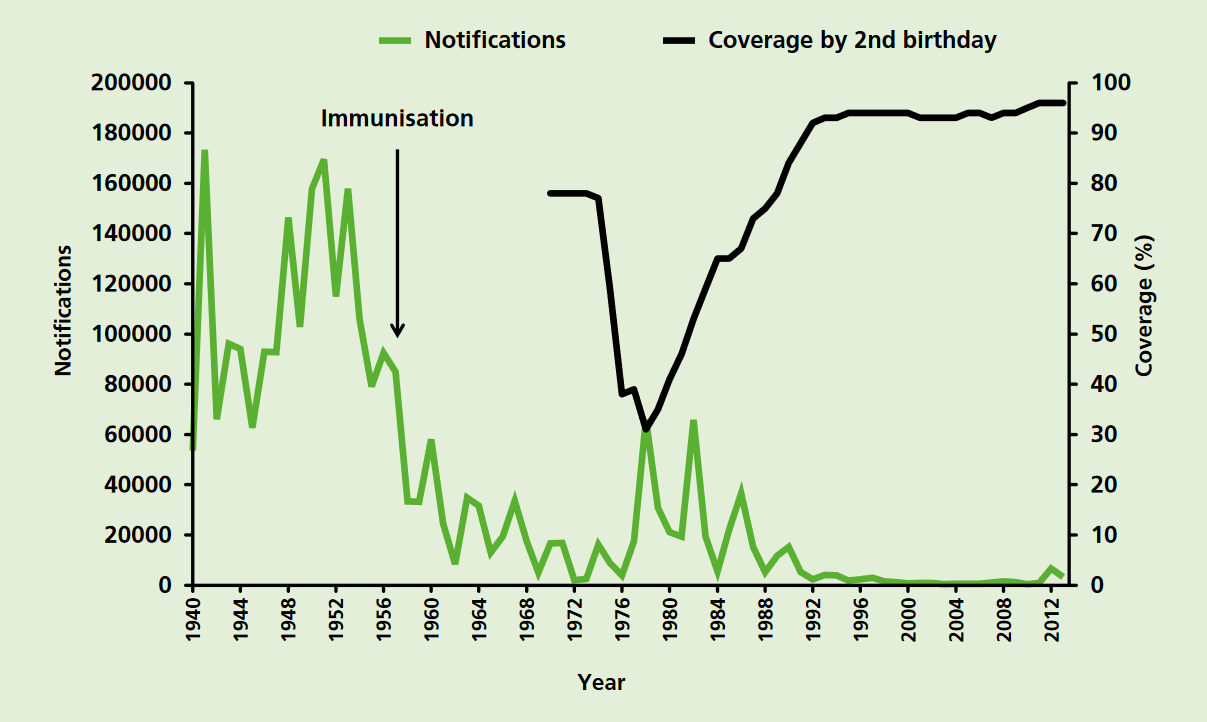
However, negative publicity and fearmongering caused the immunization rate to fall in several countries, including the UK, Sweden, and Japan. A dramatic increase in the incidence of pertussis followed. For example, in England and Wales before the introduction of pertussis immunisation in the 1950s, the average annual number of notifications exceeded 120,000. By 1972, when vaccine coverage was around 80%, there were only 2,069 notifications of pertussis. The professional and public anxiety about the safety and efficacy of the whole-cell vaccine caused coverage to fall to about 60% in 1975 and around 30% by 1978. Major epidemics occurred in 1977–79 and 1981–83. In 1978 there were over 65,000 notifications and 12 deaths (see the chart of pertussis notifications). These two major epidemics illustrate the impact of a fall in coverage of an effective vaccine. The actual number of deaths due to these pertussis outbreaks was higher since not all cases in infants are recognised.
In the United States, low-profit margins and an increase in vaccine-related lawsuits led many manufacturers to stop producing the DPT vaccine by the early 1980s. In 1982, the television documentary DPT: Vaccine Roulette by reporter Lea Thompson of Washington, D. C. station WRC-TV depicted the lives of children whose severe disabilities were incorrectly blamed on the DPT vaccine. The ensuing negative publicity led to many lawsuits against vaccine manufacturers. By 1985, vaccine manufacturers had difficulty obtaining liability insurance. The price of the DPT vaccine skyrocketed, leading providers to curtail purchases, and limiting availability. Only one manufacturer remained in the US by the end of 1985. In response, Congress passed the National Childhood Vaccine Injury Act (NCVIA) in 1986, establishing a federal no-fault system to compensate victims of injury caused by recommended vaccines.
Concerns about side effects led Sato to introduce an even safer acellular vaccine for Japan in 1981, which was approved in the US in 1992, for use in the combination DTaP vaccine. The acellular vaccine has a rate of adverse events similar to that of a Td vaccine (a tetanus-diphtheria vaccine containing no pertussis vaccine).
References
References
- (August 2015). "Pertussis vaccines: WHO position paper – September 2015". Relevé Épidémiologique Hebdomadaire.
- (2017). "The immunological basis for immunization series: module 4: pertussis, update 2017". World Health Organization.
- (September 2014). "Acellular vaccines for preventing whooping cough in children". The Cochrane Database of Systematic Reviews.
- (2012). "Introduction to Epidemiology: Distribution and Determinants of Disease". Nelson Education.
- (2025). "The selection and use of essential medicines, 2025: WHO Model List of Essential Medicines, 24th list". World Health Organization.
- (April 2014). "Pertussis resurgence: waning immunity and pathogen adaptation - two sides of the same coin". Epidemiology and Infection.
- (September 2012). "Resurgence of pertussis calls for re-evaluation of pertussis animal models". Expert Review of Vaccines.
- (28 September 2020). "Pertussis: a tale of two vaccines". Nature Research.
- (October 2000). "Pertussis infection in fully vaccinated children in day-care centers, Israel". Emerging Infectious Diseases.
- (August 2015). "Pertussis Vaccines:WHO Position Paper".
- "Immunisation and Pentavalent Vaccine". [[UNICEF]].
- (October 2013). "Pertussis: a reemerging infection". American Family Physician.
- (28 September 2012). "Whooping cough outbreak: Pregnant women to be vaccinated". [[BBC News]].
- "Tetanus Toxoid, Reduced Diphtheria Toxoid and Acellular Pertussis Vaccine Adsorbed, Adacel, Aventis Pasteur Ltd".
- (August 2013). "Public health. The pertussis paradox". Science.
- (21 May 2015). "Pertussis". [[World Health Organization]].
- (June 2023). "Diphtheria Tetanus and Pertussis Containing Vaccines: Market and Supply Update".
- (27 October 2023). "Infanrix".
- (27 October 2023). "Boostrix".
- (22 July 2022). "Daptacel".
- (27 October 2023). "Adacel".
- (27 April 2023). "Pediarix".
- (2 April 2018). "Pediarix Vaccine Questions and Answers for Healthcare Providers".
- (27 October 2023). "Kinrix".
- (22 July 2022). "Quadracel".
- (13 April 2023). "Vaxelis".
- (24 October 2022). "Pentacel".
- (August 2010). "Pearl Kendrick, Grace Eldering, and the pertussis vaccine". Emerging Infectious Diseases.
- (2013). "Pertussis: challenges today and for the future". PLOS Pathogens.
- (August 1996). "A cellular pertussis vaccine (Infanrix-DTPa; SB-3). A review of its immunogenicity, protective efficacy and tolerability in the prevention of Bordetella pertussis infection". Drugs.
- (2009). "Hot Topics in Infection and Immunity in Children V".
- Huber, Peter. (8 July 1991). "Junk Science in the Courtroom".
- Cherry, James D.. (March 2007). "Historical Perspective on Pertussis and Use of Vaccines to Prevent It: 100 years of pertussis (the cough of 100 days)".
- (1990). "'Pertussis vaccine encephalopathy': it is time to recognize it as the myth that it is". JAMA.
- (January 1998). "Impact of anti-vaccine movements on pertussis control: the untold story". Lancet.
- (21 January 2021). "Immunisation against infectious disease". Public Health England.
- Rachel K. Sobel. (22 May 2011). "At last: Ignorance inoculation". Philadelphia Inquirer.
- (28 April 1982). "TV Report On Vaccine Stirs Bitter Controversy". The Washington Post.
- (March 2006). "Update on vaccine liability in the United States: presentation at the National Vaccine Program Office Workshop on strengthening the supply of routinely recommended vaccines in the United States, 12 February 2002". Clinical Infectious Diseases.
- (August 1988). "National Childhood Vaccine Injury Compensation Act". Pediatrics.
- (June 2005). "Combined tetanus, diphtheria, and 5-component pertussis vaccine for use in adolescents and adults". JAMA.
This article was imported from Wikipedia and is available under the Creative Commons Attribution-ShareAlike 4.0 License. Content has been adapted to SurfDoc format. Original contributors can be found on the article history page.
Ask Mako anything about Pertussis vaccine — get instant answers, deeper analysis, and related topics.
Research with MakoFree with your Surf account
Create a free account to save articles, ask Mako questions, and organize your research.
Sign up freeThis content may have been generated or modified by AI. CloudSurf Software LLC is not responsible for the accuracy, completeness, or reliability of AI-generated content. Always verify important information from primary sources.
Report