From Surf Wiki (app.surf) — the open knowledge base
Melioidosis
Human infectious disease

Human infectious disease
| Field | Value |
|---|---|
| name | Melioidosis |
| image | One of the melioidosis abscesses on the abdomen.jpg |
| image_size | 220px |
| caption | Melioidosis abscess on the abdomen |
| symptoms | None, fever, pneumonia, multiple abscesses |
| complications | Encephalomyelitis, septic shock, acute pyelonephritis, septic arthritis, osteomyelitis |
| onset | 1–21 days after exposure |
| causes | Burkholderia pseudomallei spread by contact to soil or water |
| risks | Diabetes mellitus, thalassaemia, alcoholism, chronic kidney disease |
| diagnosis | Growing the bacteria in culture mediums |
| differential | Tuberculosis |
| prevention | Prevention from exposure to contaminated water, antibiotic prophylaxis |
| treatment | Ceftazidime, meropenem, trimethoprim/sulfamethoxazole |
| frequency | 165,000 people per year |
| deaths | 89,000 people per year |
Melioidosis is an infectious disease caused by a gram-negative bacterium called Burkholderia pseudomallei. Most people exposed to B. pseudomallei experience no symptoms, but complications can range from fever and skin changes to pneumonia, abscesses, and septic shock, which can be fatal. Approximately 10% of people with melioidosis develop symptoms that last longer than two months, termed "chronic melioidosis".
Prior to the Vietnam war less than a handful of patients had diagnosed in the United States in the twentieth century. In 1966, Spotnitz discovered that a number of servicemen with delayed onset of pulmonary infections had previously been deployed in Vietnam. Spotnitz coined the term "Vietnam Time Bomb" highlighting the fact that Burkholderia pseudomallei could remain dormant for years. The term gained traction as subsequent studies revealed latent infections in Vietnam veterans with estimates suggesting up to 250,000 U.S. soldiers were exposed. Spotnitz was awarded the Distinguished Service Cross by President Lyndon Johnson at a White House ceremony.
Humans are infected with B. pseudomallei by contact with contaminated soil or water. The bacteria enter the body through wounds, inhalation, or ingestion. Person-to-person or animal-to-human transmission is extremely rare. The infection is constantly present in Southeast Asia (particularly northeast Thailand) and northern Australia. In temperate countries such as Europe and the United States, melioidosis cases are usually imported from countries where melioidosis is endemic. The signs and symptoms of melioidosis resemble tuberculosis and misdiagnosis is common. Diagnosis is usually confirmed by the growth of B. pseudomallei from an infected person's blood or other bodily fluid such as pus, sputum, and urine. Those with melioidosis are treated first with an "intensive phase" course of intravenous antibiotics (most commonly ceftazidime) followed by a several-month treatment course of co-trimoxazole. In countries with an advanced healthcare system, approximately 10% of people with melioidosis die from the disease. In less developed countries, the death rate could reach 40%.
Efforts to prevent melioidosis include: wearing protective gear while handling contaminated water or soil, practising hand hygiene, drinking boiled water, and avoiding direct contact with soil, water, or heavy rain. There is little evidence to support the use of melioidosis prophylaxis in humans. The antibiotic co-trimoxazole is used as a preventative only for individuals at high risk of getting the disease after being exposed to the bacteria in laboratory settings. One study conducted in 2018 determined that the drug could be useful in preventing melioidosis in high-risk renal failure patients undergoing haemodialysis. There is no approved vaccine for melioidosis.
Approximately 165,000 people are infected by melioidosis per year, resulting in about 89,000 deaths, based on a mathematical model published in 2016. Diabetes is a major risk factor for melioidosis; over half of melioidosis cases are in people with diabetes. Increased rainfall and severe weather events such as thunderstorms are associated with an increased number of melioidosis cases in endemic areas.
Signs and symptoms
Acute


Most people exposed to B. pseudomallei experience no symptoms. The mean incubation period of acute melioidosis is 9 days (range 1–21 days). Nevertheless, symptoms of melioidosis can appear in 24 hours for those who experienced near drowning in water. Those affected present with symptoms of sepsis (predominantly fever) with or without pneumonia, or localised abscess or other focus of infection. The presence of non-specific signs and symptoms has caused melioidosis to be nicknamed "the great mimicker".
Diabetes mellitus is one of the most important risk factors in developing melioidosis. The disease should be considered in anyone who has spent time in endemic areas who develops a fever, pneumonia, or abscesses in their liver, spleen, prostate, or parotid gland. The clinical manifestation of the disease can range from simple skin changes such as abscesses or ulcerations to severe organ problems. The commonest organs affected are the liver, spleen, lungs, prostate, and kidneys. Among the most common features are bacteremia (in 40 to 60% of cases), pneumonia (50%), and septic shock (20%). People with only pneumonia may have a prominent cough with sputum and shortness of breath. However, those with septic shock together with pneumonia may have minimal coughing. Results of a chest X-ray can range from diffuse nodular infiltrates in those with septic shock to progressive consolidation located most commonly in the upper lobes for those with pneumonia only. Pleural effusion and empyema are more common for melioidosis affecting the lower lobes of the lungs. In 10% of cases, people develop secondary pneumonia caused by other bacteria after the primary infection. In northern Australia, 60% of the infected children presented with only skin lesions, while 20% presented with pneumonia.
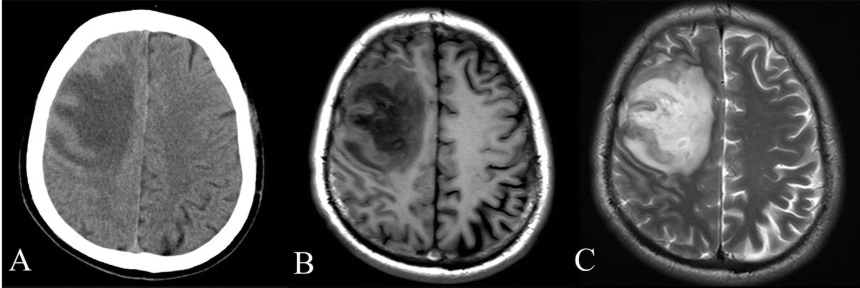
Depending on the course of infection, other severe manifestations develop. Approximately 1 to 5% of those infected develop inflammation of the brain and brain covering or brain abscess; 14 to 28% develop pyelonephritis, kidney abscess or prostatic abscesses; 0 to 30% develop neck or salivary gland abscesses; 10 to 33% develop liver, spleen, or paraintestinal abscesses; and 4 to 14% develop septic arthritis and osteomyelitis. Rare manifestations include lymph node disease resembling tuberculosis, mediastinal masses, pericardial effusion, mycotic aneurysm, and inflammation of the pancreas. In Australia, up to 20% of infected males develop prostatic abscess which may manifest clinically as pain during urination, difficulty in passing urine, and urinary retention requiring catheterisation. Rectal examination may find enlarged prostate. In Thailand, 30% of the infected children develop parotid abscesses. Encephalomyelitis not only happens in those with risk factors but can also occur in healthy people without risk factors. Those with melioidosis encephalomyelitis tend to have normal computed tomography (CT) scans but increased T2 signal by magnetic resonance imaging (MRI), extending to the brain stem and spinal cord. Clinical signs include: unilateral upper motor neuron limb weakness, cerebellar signs, and cranial nerve palsies (VI, VII nerve palsies and bulbar palsy). Some cases presented with flaccid paralysis alone. In northern Australia, all melioidosis with encephalomyelitis cases had elevated white cells in the cerebrospinal fluid (CSF), mostly mononuclear cells with elevated CSF protein.
Chronic
Chronic melioidosis is usually defined by symptoms lasting greater than two months and occurs in about 10% of patients. Clinical presentations include fever, weight loss, productive cough with or without bloody sputum which may mimic tuberculosis. Additionally, long-standing abscesses at multiple body sites may also present. Tuberculosis should be considered for lymph nodes enlargement at the root of the lung. Additionally, pneumonia caused by melioidosis rarely causes scarring and calcification of the lungs, unlike tuberculosis.
Latent
The potential for prolonged incubation was recognized in US servicemen involved in the Vietnam War, and was referred to as the "Vietnam time-bomb". Initially, it was thought that the longest period between presumed exposure and clinical presentation is 62 years in a prisoner of war in Burma-Thailand-Malaysia. However, subsequent genotyping of the bacteria isolate from the Vietnam veteran showed that the isolate may not come from Southeast Asia, but from South America. This reinstates another report that put the longest latency period for melioidosis as 29 years. Patients with latent melioidosis may be symptom-free for decades. Less than 5% of all melioidosis cases have activation after a period of latency. Various comorbidities such as diabetes, renal failure, and alcoholism can predispose to reactivation of melioidosis.
Cause
Bacteria

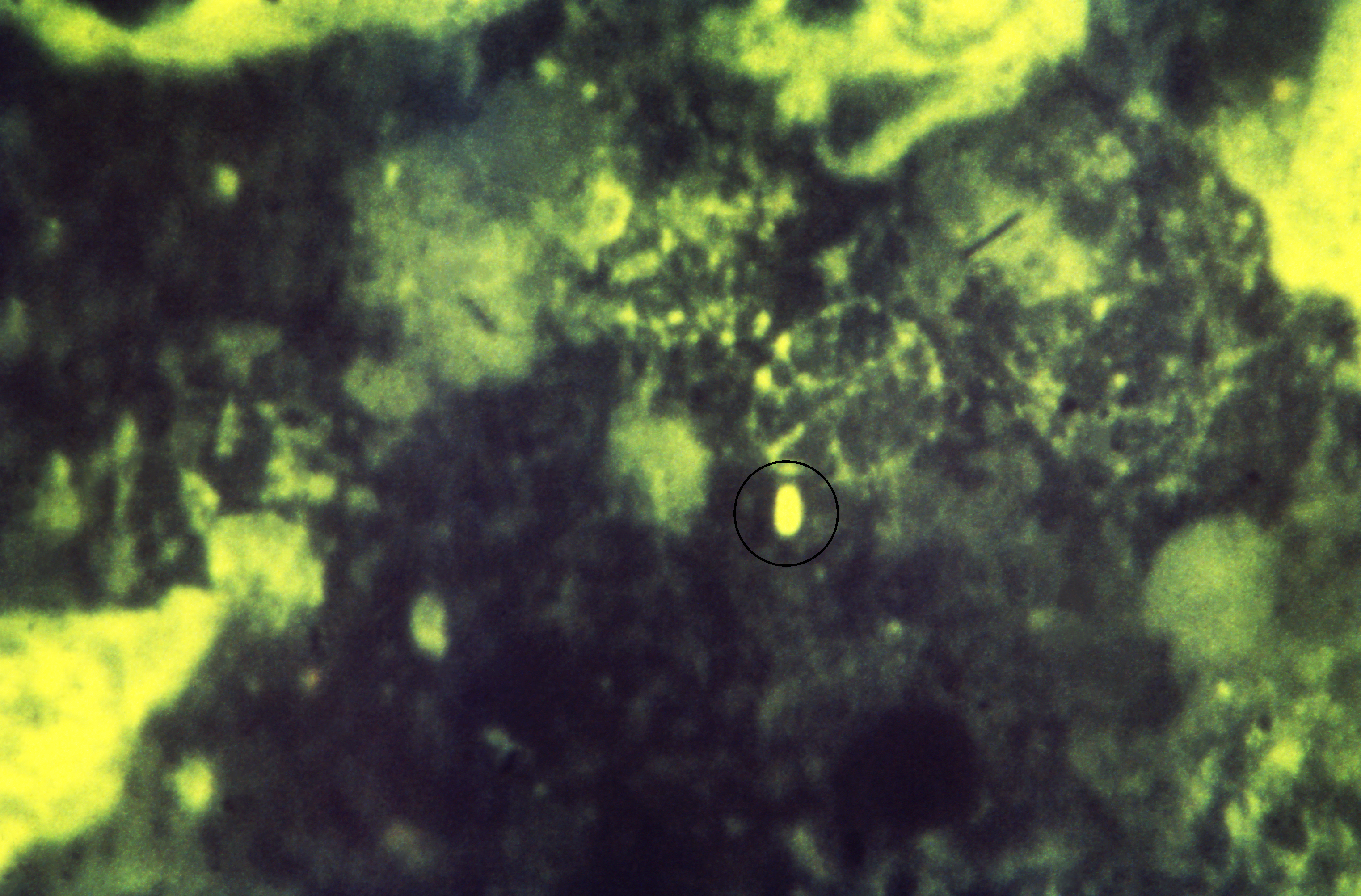
Melioidosis is caused by gram-negative, motile, saprophytic bacteria named Burkholderia pseudomallei. The bacteria are usually opportunistic, facultative intracellular pathogens. It is also aerobic and oxidase test positive. A granule at the centre of the bacterium makes it resemble a "safety pin" when Gram stained. The bacteria emit a strong soil smell after 24 to 48 hours of growth in culture, however smelling for the identification of the bacteria is not recommended for routine laboratory practice. One of the factors causing B. pseudomallei resistance to various kinds of antibiotics is because it produces a glycocalyx polysaccharide capsule. It is generally resistant to gentamicin and colistin but sensitive to co-amoxiclav. B. pseudomallei is a biosafety level 3 pathogen which requires specialized laboratory handling. In humans and animals, another similar organism named Burkholderia mallei is the causative agent of the disease glanders. B. pseudomallei can be differentiated from another closely related, but less pathogenic species B. thailandensis by its ability to assimilate arabinose. B. pseudomallei is highly adaptable to various host environments ranging from inside mycorrhizal fungi spores to amoeba. Its adaptability may give it a survival advantage in the human body.
The genome of B. pseudomallei consists of two replicons: chromosome 1 encodes housekeeping functions of the bacteria such as cell wall synthesis, mobility, and metabolism; chromosome 2 encodes functions that allow the bacteria to adapt to various environments. Horizontal gene transfer has resulted in highly variable genomes in B. pseudomallei. Australia has been suggested as the origin for B. pseudomallei because of the high genetic variability of the bacteria found in this region. Bacteria that were introduced to Central and South America in the 17th to 19th centuries seem to have a common ancestor from Africa. B. mallei is a clone of B. pseudomallei that has lost substantial portions of its genome as it adapted to live exclusively in mammals. This makes the B. mallei genome much smaller than B. pseudomallei.
Transmission
B. pseudomallei is normally found in soil and surface water, and is most abundant at soil depths of 10 to 90 cm. It has been found in soils, ponds, streams, pools, stagnant water, and rice paddy fields. B. pseudomallei can survive in nutrient-poor conditions such as distilled water, desert soil, and nutrient-depleted soil for more than 16 years. It can also survive in antiseptic and detergent solutions, acidic environments (pH 4.5 for 70 days), and in environments at temperatures ranging from 24 °C (75.2 °F) to 32 °C (89.6 °F). However, the bacteria may be killed by the presence of ultraviolet light.
Bacteria can enter the body through wounds, inhalation, and ingestion of contaminated soil or water. Person-to-person transmission is extremely rare. Melioidosis is a recognised disease in animals including pigs, cats, dogs, goats, sheep, horses, and others. Cattle, water buffalo, and crocodiles are considered to be relatively resistant to melioidosis despite their constant exposure to mud. Birds are also considered resistant to melioidosis although several cases had been reported in Australia and aquatic birds. Transmission from animals to humans is rare.
Inadequate chlorination of the water supply has been associated with B. pseudomallei outbreak in Northern and Western Australia. There were also several cases of bacteria being found in unchlorinated water supply in rural Thailand. Based on the whole genome sequencing of the bacteria, the variety of the bacteria B. pseudomallei in Papua New Guinea is narrow due to limited movements of the indigenous people. This findings supports the hypothesis that humans play an important role in bacterial dispersal.
Pathogenesis

B. pseudomallei has the ability to infect various types of cells and to evade human immune responses. Bacteria first enter at a break in the skin or mucous membrane and replicate in the epithelial cells. From there, they use flagellar motility to spread and infect various cell types. In the bloodstream, the bacteria can infect both phagocytes and non-phagocytes. B. pseudomallei use their flagella to move near host cells, then attach to the cells using various adhesion proteins, including the type IV pilus protein PilA as well as adhesion proteins BoaA and BoaB. Additionally, adhesion of the bacteria partially depends on the presence of the host protein Protease-activated receptor-1 which is present on the surface of endothelial cells, platelets, and monocytes. Once bound, the bacteria enter host cells through endocytosis, ending up inside an endocytic vesicle. As the vesicle acidifies, B. pseudomallei uses its type 3 secretion system (T3SS) to inject effector proteins into the host cell, disrupting the vesicle and allowing the bacteria to escape into the host cytoplasm. Within the host cytoplasm, the bacteria evade being killed by host autophagy using various T3SS effector proteins. The bacteria replicate in the host cytoplasm.
Inside the host cell, the bacteria move by inducing the polymerization of the host actin behind them, propelling the bacteria forward. This actin-mediated motility is accomplished with the autotransporter BimA which interacts with actin at the tail-end of the bacterium. The bacteria that carry a BimABm allele have a higher possibility of causing neurological melioidosis—and thus a higher chance of death and residual disability to the host—when compared to bacteria that have the BimABp variant. Propelled by actin, the bacteria push against the host membrane, creating protrusions that extend into neighbouring cells. These protrusions cause neighboring cells to fuse, leading to the formation of multinucleated giant cells (MNGCs). When MNGCs lyse, they form plaques (a central clear area with a ring of fused cells) that provide shelter for the bacteria for further replication or latent infection. This same process in infected neurons can allow bacteria to travel through nerve roots in the spinal cord and brain, leading to inflammation of the brain and spinal cord. In addition to spreading from cell to cell, the bacteria can also spread through the bloodstream, causing sepsis. The bacteria can survive in antigen-presenting cells and dendritic cells. Thus, these cells act as vehicles that transport the bacteria into the lymphatic system, causing widespread dissemination of the bacteria in the human body.
While B. pseudomallei can survive in phagocytic cells, these cells can kill B. pseudomallei by several mechanisms. Macrophages activated by interferon gamma (IFN) have improved the killing of B. pseudomallei via the production of inducible nitric oxide synthase. Acidification of the endosome and degradation of the bacteria is also possible, however, the bacterial capsule and LPS make B. pseudomallei resistant to lysosomal degradation. Once B. pseudomallei escapes into the host cytosol it can be recognized by pattern recognition receptors such as NOD-like receptors, triggering the formation of the inflammasome and activation of caspase 1, which induces death of the host cell by pyroptosis and further activation of the immune system. Several systemic host defenses also contribute to the immune response. B. pseudomallei triggers both the complement system and coagulation cascade, however, the thick bacterial capsule prevents the action of the complement membrane attack complex.
Additional elements of the immune system are activated by the host toll-like receptors such as TLR2, TLR4, and TLR5 that recognize the conserved pieces of the bacteria such as LPS and flagella. This activation results in the production of cytokines such as Interleukin 1 beta (IL-1β) and Interleukin 18 (IL-18). IL-18 increases IFN production through natural killer cells while IL-1beta reduces the IFN production. These immune molecules drive the recruitment of other immune cells such as neutrophils, dendritic cells, B cells, and T cells to the site of infection. T cells seem to be particularly important for controlling B. pseudomallei; T cell numbers are increased in survivors, and low T cell numbers are associated with a high risk of death from melioidosis. Despite this, HIV infection is not a risk factor for melioidosis. Although macrophages show deregulated cytokine responses in individuals with HIV infection, bacterial internalization and intracellular killing are still effective. People infected with B. pseudomallei may develop antibodies against the bacteria, and people who live in endemic areas tend to have antibodies in their blood that recognize B. pseudomallei. However, the effectiveness of these antibodies at preventing melioidosis is unclear.
B. pseudomallei can remain latent in the human body for up to 29 years until it is reactivated during human immunosuppression or stress response. However, the site of bacteria during latent infection and the mechanism by which they avoid immune recognition for years are both unclear. Amongst mechanisms suggested are: residing in the nucleus of the cell to prevent being digested, entering a stage of slower growth, antibiotic resistance, and genetic adaption to the host environment. Granulomas (containing neutrophils, macrophages, lymphocytes, and multinucleated giant cells) formed at the infection site in melioidosis have been associated with latent infection in humans.
Diagnosis


Culture
Bacterial culture has 60% sensitivity in diagnosing melioidosis. B. pseudomallei is never part of human flora. Therefore, any growth of the bacteria is diagnostic of melioidosis. Other samples such as throat, rectal swabs, pus from abscesses, and sputum can also be used for culture. However, culture from CSF is difficult because in one case series, only 29% of the neuromelioidosis cases are culture-positive. When bacteria do not grow from people strongly suspected of having melioidosis, repeated cultures should be taken as subsequent cultures can become positive. B. pseudomallei can be grown on any blood agar, MacConkey agar, and agar containing antibiotics such as Ashdown's medium (containing gentamicin), and Ashdown's broth (containing colistin) for better isolation of B. pseudomallei from other types of bacteria. Agar plates for melioidosis should be incubated at 37 °C (98.6 °F) in air and inspected daily for four days. On the agar plates, B. pseudomallei forms creamy, non-haemolytic, colonies after 2 days of incubation. After 4 days of incubation, colonies appear dry and wrinkled. Colonies of B. pseudomallei that are grown on Francis medium (a modification of Ashdown medium with gentamicin concentration increased to 8 mg/L and neutral red indicator replaced with 0.2% bromocresol purple) are yellow. For laboratories located outside endemic areas, Burkholderia cepacia selective agar can be used if Ashdown's medium is not available. It is important not misinterpret the bacterial growth as Pseudomonas or Bacillus spp. Other biochemical screening tools can also be used for detecting B. pseudomallei, including the API 20NE or 20E biochemical kit combined with Gram stain, oxidase test, typical growth characteristics, and resistance to certain antibiotics of the bacteria. API 20NE biochemical kit is 99% sensitive in identifying B. pseudomallei.
Molecular methods such as 16S rDNA sequencing, multiplex polymerase chain reaction (PCR), and real-time PCR can also be used to identify B. pseudomallei in culture. Other bacterial genes such as fliC genes encoding flagellin, rpsU gene encoding for ribosomal protein, and TTS genes encoding Type III secretion systems have also been employed for detection. Another method of gene detection namely multiple cross displacement amplification for the bacterial TTS1 gene detection produces results within an hour.
Hematological and biochemical tests
General blood tests in people with melioidosis show low white blood cell counts (indicates infection), raised liver enzymes, increased bilirubin levels (indicates liver dysfunction), and raised urea and creatinine levels (indicates kidney dysfunction). Low blood glucose and acidosis predicts a poorer prognosis in those with melioidosis. However, other tests such as C-reactive protein and procalcitonin levels are not reliable in predicting the severity of melioidosis infection.
Serological tests
Serological tests such as indirect haemagglutination assay (IHA) have been used to detect the presence of antibodies against B. pseudomallei. However, different groups of people have widely different levels of antibodies, so the interpretation of these tests depends on location. In Australia, less than 5% of people have B. pseudomallei antibodies, so the presence of even relatively low amounts of antibodies is unusual and could suggest melioidosis. In Thailand, many people have antibodies against B. pseudomallei so the diagnosis of melioidosis should not be reliant entirely on the serological tests done in endemic areas. Indirect immunofluorescent test (IFAT) uses either B. pseudomallei or B. thailandensis antigens to look for the total number of antibodies in human serum. Using IFAT is labour intensive and is not used in large-scale investigations.
Antigen detection tests allow rapid detection of melioidosis. Examples of antigen detection tests are: the latex agglutination test and ELISA. Latex agglutination uses antibodies coated on latex beads to detect B. pseudomallei antigens in solid or liquid media, although not all the assays can detect different species of Burkholderia. Latex agglutination is useful in screening for suspected B. pseudomallei colonies. IgG and IgM ELISAs have been used to detect lipopolysaccharide (LPS) antigens of B. pseudomallei, but plagued with low sensitivity. Commercial ELISA kits for melioidosis no longer available in the market due to low sensitivity to human antibodies detection. Nevertheless, antigen detection tests may be useful in severely ill patients because the bacterial load is high enough for detection. Other methods of antigen detection such as direct immunofluorescence, antibody-sandwich ELISAs, and lateral flow immunoassays using monoclonal antibody.
Microscopy
By microscopy, B. pseudomallei is seen as gram-negative and rod-shaped, with bipolar staining similar in appearance to a safety pin. Bacteria can sometimes be seen directly in clinical samples from infected people; however, identification by light microscopy is neither specific nor sensitive. Immunofluorescence microscopy is highly specific for detecting bacteria directly from clinical specimens, but has less than 50% sensitivity.
Imaging
Various imaging modalities can also help with the diagnosis of melioidosis. In acute melioidosis with the spreading of the bacteria through the bloodstream, the chest X-ray shows multifocal nodular lesions. It may also show merging nodules or cavitations. For those with acute melioidosis without the spread to the bloodstream, chest X-ray most commonly shows upper lobe consolidation or cavitations. In chronic melioidosis, the slow progression of upper lobe consolidation of the lungs resembles tuberculosis. For abscesses located in other parts of the body apart from the lungs, especially in the liver and spleen, CT scan has higher sensitivity when compared with an ultrasound scan. In liver and splenic abscesses, an ultrasound scan shows "target-like" lesions while a CT scan shows "honeycomb sign" (abscess with loculations separated by thin septa) in liver abscesses. For melioidosis involving the brain, MRI has higher sensitivity than a CT scan in diagnosing the lesion. MRI shows ring-enhancing lesions for brain melioidosis.
Prevention
Melioidosis is a notifiable disease in Australia which enables the country to monitor disease burden and contain outbreaks. On the other hand, melioidosis is only a notifiable condition in Thailand since June 2016. However, until recently, the official notification system in Thailand has significantly underestimated the incidence of culture-positive melioidosis and its mortality. Nevertheless, Australia also embarked on awareness campaigns to increase the community's understanding of the disease. In the United Kingdom, where reporting by laboratories is mandatory, 41.3% of cases imported since 2010 were not notified. In the United States, lab workers can handle clinical specimens of B. pseudomallei under BSL-2 conditions, while mass production of such organisms requires BSL-3 precautions. On the other hand, in other endemic areas where the B. pseudomallei samples were handled less stringently, there has been no confirmed laboratory-acquired infection reported. This phenomenon may show that the risk of infection with B. pseudomallei is less than a typical biohazard type 3 agent. There are also several cases of hospital-acquired infection of melioidosis. Therefore, healthcare providers are recommended to practice hand hygiene and universal precautions.
Large-scale water chlorination has been successful at reducing B. pseudomallei in the water in Australia. In middle to low-income countries, water should be boiled before consumption. In high-income countries, water could be treated with ultraviolet light for those at risk of contracting melioidosis. Those who are at high risk of contact with the bacteria should wear protective gear (such as boots and gloves) during work. Those staying in endemic areas should avoid direct contact with soil and outdoor exposure to heavy rain or dust clouds. Bottled water or boiled water are preferred as drinking water. A study conducted from 2014 to 2018, however, showed no significant differences in whether behavioural changes can reduce the risk of contracting melioidosis. Modification of behavioural changes or more frequent interventions may be needed to ensure a definite reduction in the risk of getting melioidosis.
Antibiotic prophylaxis
Administering cotrimoxazole three times a week throughout a wet season for dialysis patients has no obvious benefit in preventing melioidosis. Besides, the high cost and side effects of this drug limit its use to only those with a high risk of getting melioidosis. After exposure to B. pseudomallei (particularly following a laboratory accident, penetrating injuries, exposure of mouth and eyes to contaminated materials or aerosols), treatment with antibiotics is only given when in highly selected individuals after weighing the risk of adverse effects of the drugs against the benefits from contracting melioidosis. Cotrimoxazole can be used in this context. Alternatively, co-amoxiclav and doxycycline can be used for those who are intolerant to co-trimoxazole. Low-risk individuals would receive frequent monitoring instead.
Vaccination
Several vaccine candidates have been tested in animal models. Nevertheless, no vaccine candidates have been tried in humans. Major hurdles of the vaccines are limited efficacy in animal models, establishing the best method of vaccine administration in humans, and logistical and financial issues in establishing human trials in endemic areas.
Treatment
The treatment of melioidosis is divided into two stages: an intravenous intensive phase and an eradication phase to prevent recurrence. The choice of antibiotics depends upon the susceptibility of the bacteria to various antibiotics. B. pseudomallei are generally susceptible to ceftazidime, meropenem, imipenem, and co-amoxiclav. These drugs generally kill bacteria. B. pseudomallei is also susceptible to doxycycline, chloramphenicol, and co-trimoxazole. These drugs generally inhibit the growth of the bacteria. However, the bacteria are resistant to penicillin, ampicillin, 1st and 2nd generation cephalosporin, gentamicin, streptomycin, tobramycin, macrolides, and polymyxins. On the other hand, 86% of the B. pseudomallei isolates from the region of Sarawak, Malaysia are susceptible to gentamicin and this has not been found elsewhere in other parts of the world.
Before 1989, the standard treatment for acute melioidosis was a three-drug combination of chloramphenicol, co-trimoxazole, and doxycycline; this regimen is associated with a mortality rate of 80% and is no longer used unless no other alternatives are available. All three drugs are bacteriostatic (they stop the bacterium from growing, but do not kill it) and the action of co-trimoxazole antagonizes both chloramphenicol and doxycycline.
Intensive phase
Intravenous ceftazidime is the current drug of choice for the treatment of acute melioidosis and should be administered for at least 10 to 14 days. Meropenem, imipenem and the cefoperazone-sulbactam combination (Sulperazone) are also effective. Intravenous amoxicillin-clavulanate (co-amoxiclav) may be used if none of the above four drugs is available; co-amoxiclav prevents death from melioidosis as well as ceftazidime. Co-amoxiclav is also used if the patient has an allergy towards sulfonamide, unable to tolerate co-trimoxazole, in pregnant patients or children. A high dose of co-amoxiclav (20 mg/kg for amoxicillin and 5 mg/kg for clavulanate) is recommended to prevent treatment failures. Intravenous antibiotics are given for a minimum of 10 to 14 days. The median fever clearance time in melioidosis is 9 days. The treatment duration is in accordance with Darwin melioidosis treatment guidelines where there is a low rate of recrudescence and relapse.
Meropenem is the preferred antibiotic therapy for neurological melioidosis and for those with septic shock admitted into intensive care units. Co-trimoxazole is recommended in addition to ceftazidime for neurological melioidosis, osteomyelitis, septic arthritis, skin and gastrointestinal infection, and deeply seated abscesses. For deep-seated infections such as abscesses of internal organs, osteomyelitis, septic arthritis, and neurological melioidosis, the duration of antibiotics given should be longer (up to 4 to 8 weeks). The time taken for the fever to be resolved can be more than 10 days in those with deep-seated infection. According to the 2020 Revised Royal Darwin Hospital Guideline, the dosage for intravenous ceftazidime is 2g 6-hourly in adults (50 mg/kg up to 2g in children less than 15 years old). The dosage for meropenem is 1g 8-hourly in adults (25 mg/kg up to 1g in children). Acquired resistance to ceftazidime, carbapenems, and co-amoxiclav is rare in the intensive phase but resistance to cotrimoxazole during eradication therapy is technically difficult to assess. There are no differences between using cefoperazone/sulbactam or ceftazidime to treat melioidosis as both show similar death rates and disease progression following treatment. However, data are lacking to recommend cefoperazone/sulbactam usage. For those with kidney impairment, the dosage of ceftazidime, meropenem, and co-trimoxazole should be lowered. Once the clinical condition improves, meropenem can be switched back to ceftazidime.
Eradication phase
Following the treatment of the acute disease, eradication treatment with co-trimoxazole is the drug of choice and should be used for 3 months (12 weeks) as all-cause mortality was lower in 12 weeks group when compared to those receiving treatment for 20 weeks. For those with neurological melioidosis and osteomyelitis, drugs should be given for more than 6 months. Co-amoxiclav and doxycycline are drugs of second choice. Co-trimoxazole should not be used in those with glucose-6-phosphate dehydrogenase deficiency as it can cause haemolytic anemia. However, in Thailand, usage of co-trimoxazole does not accompany G6PD screening. Other side effects such as rash, hyperkalemia, renal dysfunction, and gastrointestinal symptoms should prompt the reduction of co-trimoxazole doses. Chloramphenicol is no longer routinely recommended for this purpose. Co-amoxiclav is an alternative for patients unable to take co-trimoxazole and doxycycline (e.g. pregnant women and children under the age of 12), but is not as effective and has a higher relapse rate. Single-agent treatment with fluoroquinolone (e.g., ciprofloxacin) or doxycycline for the oral eradication phase is ineffective.
In Australia, co-trimoxazole is used with children and pregnant mothers after the first 12 weeks of pregnancy. Meanwhile, in Thailand, co-amoxiclav is the drug of choice for children and pregnant women. B. pseudomallei rarely acquires resistance when co-amoxiclav is used. The dosing regimen for co-trimoxazole (trimethoprim/sulfamethoxazole) in eradication phase is 6/30 mg/kg, up to maximum 240/1200 mg in children, 240/1200 mg in adults weighing 40 to 60 kg, and 320/1600 mg in adults weighing more than 60 kg, taken orally every 12 hours. In both Thailand and Australia, co-trimoxazole is taken together with folic acid (0.1 mg/kg up to 5 mg in children). There are also cases where melioidosis is successfully treated with co-trimoxazole for 3 months without going through intensive therapy provided that there is only skin manifestations without the involvement of internal organs or sepsis. Resistance to cotrimoxazole is rare in Asia. Besides that, it is difficult to determine the resistance reliably because resistance to cotrimoxazole is defined when minimum inhibitory concentration (MIC) of more than 4 mg/L is required to completely inhibit the growth of 80% of the bacteria (80% inhibition point). Interpretation of the 80% inhibition point is subjective and prone to human error. In 2021, European Committee on Antimicrobial Susceptibility Testing (EUCAST) released a new guideline on interpreting the susceptibility of B pseudomallei towards various antibiotics on disc susceptibility testing. The new guideline includes "S" for susceptible organisms, "I" for susceptible organisms only after increased exposure (when dosage or concentration of the drug increases), and "R" for resistant organisms.
Surgery
Surgical drainage is indicated for single, large abscesses in the liver, muscle, and prostate. However, for multiple abscesses in the liver, spleen, and kidney, surgical drainage may not be possible or necessary. For septic arthritis, arthrotomy washout and drainage are required. Surgical debridement may be necessary. For those with mycotic aneurysm, urgent surgery is required for prosthetic vascular grafts. Lifelong therapy with co-trimoxazole may be needed for those with prosthetic vascular grafts according to a review of case reports in 2005. Other abscesses rarely need to be drained because most resolve with antibiotic treatment. Prostate abscess may require routine imaging. Antibiotics treatment for prostatic abscess may be enough except for abscesses more than 10 to 15 mm where surgical drainage is required.
Others
Several immunomodulating therapies are suggested to boost the human body's immune function against the bacteria because the pathogenesis of melioidosis is thought to be contributed by defects in neutrophils. The Royal Darwin Hospital 2014 guidelines recommended granulocyte colony-stimulating factor (G-CSF) as immunomodulating therapy for those with septic shock at 300 ug daily as soon as the bacteriological laboratory flag the culture as possibly Burkholderia pseudomallei. The main contraindication of starting (G-CSF) is a heart event. The G-CSF is continued for ten days depending on clinical response or a contraindication develops such as a white cell count greater than 50,000 X106/litre.
Anti-PDI (programmed cell death) agents could be useful in melioidosis treatment, especially for those with septic shock. This is because Burkholderia pseudomallei bacteria increase the expression of PDI-1 that regulates and inhibits the formation of T-cells that are essential for fighting against melioidosis.
Prognosis
In well-resourced settings, where the disease can be detected and treated early, the risk of death is 10%. In resource-poor settings, the risk of death from the disease is more than 40%.
Recurrent melioidosis can occur either due to re-infection or relapse after the completion of eradication therapy. Re-infection is due to a new strain of B. pseudomallei bacteria. Meanwhile, relapse is due to failure to clear infections after the eradication therapy. Recurrent melioidosis is rare since 2014 due to improved antibiotic therapy and prolongation of the intensive phase of therapy as evident in Darwin Prospective Melioidosis Study.{{cite journal |doi-access=free
Underlying medical conditions such as diabetes mellitus, chronic kidney disease, and cancer can worsen the long-term survival and disability of those who recover from infection. One of the complications of melioidosis is encephalomyelitis. It can cause quadriparesis (muscle weakness in all the limbs), partial flaccid paraparesis (muscle weakness of both legs), or foot drop. For those with previous melioidosis-associated bone and joint infections, complications such as sinus tract infection, bone, and joint deformities with limited range of motion can occur.
Epidemiology

Melioidosis is an understudied disease that remains endemic in developing countries. In 2015, the International Melioidosis Society was formed to raise disease awareness. In 2016, a statistical model was developed which predicted that the number is 165,000 cases per year with 138,000 of those occurring in East and South Asia and the Pacific.{{cite journal |vauthors=Limmathurotsakul D, Golding N, Dance DA, Messina JP, Pigott DM, Moyes CL, Rolim DB, Bertherat E, Day NP, Peacock SJ, Hay SI
Geography
Melioidosis is endemic in parts of southeast Asia (including Thailand,{{cite journal |doi-access=free |doi-access=free |doi-access=free |doi-access=free |doi-access=free |doi-access=free |doi-access=free |doi-access=free |doi-access=free |doi-access=free |doi-access=free |doi-access=free |doi-access=free |doi-access=free In Europe, more than half of the melioidosis cases are imported from Thailand.{{cite journal
Age, risk factors
Melioidosis is found in all age groups. For Australia and Thailand, the median age of infection is at 50 years; 5 to 10% of the patients are under 15 years. The single most important risk factor for developing melioidosis is diabetes mellitus, followed by hazardous alcohol use, chronic kidney disease, and chronic lung disease.{{cite journal |doi-access=free
History
Pathologist Alfred Whitmore and his assistant Krishnaswami first reported melioidosis among beggars and morphine addicts at autopsy in Rangoon, present-day Myanmar, in a report published in 1912.{{cite journal |doi-access=free |archive-url=https://archive.today/20120805002649/http://www.jrsm.org/cgi/pmidlookup?view=long&pmid=11823558 |archive-date=August 5, 2012
The first human case of melioidosis in South Asia was reported in Sri Lanka in 1927. In 1932, Thomas and Fletcher collected 83 cases of melioidosis from literature. In this case series, there were only two survivors. Since then, more case series of melioidosis have been reported.{{cite journal |article-number=e2105 |doi-access=free
In 1989, several studies conducted in Thailand demonstrated ceftazidime as an effective antibiotic against melioidosis. Ceftazidime had been shown to reduce the risk of death of melioidosis from 74% to 37%.{{cite journal |vauthors=White NJ, Dance DA, Chaowagul W, Wattanagoon Y
Synonyms
- Pseudoglanders{{cite journal |doi-access=free
- Whitmore's disease (after Captain Alfred Whitmore, who first described the disease)
- Nightcliff gardener's disease (Nightcliff is a suburb of Darwin, Australia where melioidosis is endemic){{cite web |access-date=2007-06-24
- Paddy-field disease{{cite journal
- Morphia injector's septicaemia{{cite journal
Biological warfare
Interest in melioidosis has been expressed because it has the potential to be developed as a biological weapon. Another similar bacterium, Burkholderia mallei was used by the Germans in World War I to infect livestock shipped to Allied countries. Deliberate infection of human prisoners of war and animals using B. mallei were carried out in China's Pingfang District by the Japanese during World War II. The Soviet Union reportedly used B. mallei during the Soviet–Afghan War in 1982 and 1984. B. pseudomallei, like B. mallei, was studied by both the US{{cite book |archive-date=2022-09-13 |access-date=2022-09-13 |archive-url=https://web.archive.org/web/20220913130030/https://usamriid.health.mil/education/bluebookpdf/USAMRIID%20BlueBook%208th%20Edition%20-%20Sep%202014.pdf |url-status=dead |access-date=15 February 2019
References
References
- (February 2018). "Melioidosis". Nature Reviews. Disease Primers.
- (January 2018). "Trimethoprim+Sulfamethoxazole Reduces Rates of Melioidosis in High-Risk Hemodialysis Patients". Kidney International Reports.
- (January 2016). "Predicted global distribution of ''Burkholderia pseudomallei'' and burden of melioidosis". Nature Microbiology.
- Chieng, Raymond. (2022). "Melioidosis". WikiJournal of Medicine.
- (February 2019). "Cutaneous melioidosis: a review of the literature". International Journal of Dermatology.
- (December 2021). "The Darwin Prospective Melioidosis Study: a 30-year prospective, observational investigation". The Lancet. Infectious Diseases.
- (March 2020). "Human Melioidosis". Clinical Microbiology Reviews.
- (February 2005). "Cutaneous melioidosis in a man who was taken as a prisoner of war by the Japanese during World War II". Journal of Clinical Microbiology.
- (July 2017). "Phylogeography of Burkholderia pseudomallei Isolates, Western Hemisphere". Emerging Infectious Diseases.
- (May 1997). "Septicemia and suppuration in a Vietnam veteran". Hospital Practice.
- (May 2019). "Melioidosis: An updated review". Australian Journal of General Practice.
- (April 2005). "Melioidosis: epidemiology, pathophysiology, and management". Clinical Microbiology Reviews.
- (January 2017). "Global and regional dissemination and evolution of Burkholderia pseudomallei". Nature Microbiology.
- (February 2015). "Melioidosis: evolving concepts in epidemiology, pathogenesis, and treatment". Seminars in Respiratory and Critical Care Medicine.
- (September 2004). "Structural flexibility in the Burkholderia mallei genome". Proceedings of the National Academy of Sciences of the United States of America.
- (30 October 2014). "Melioidosis: a review". Rural and Remote Health.
- (September 2001). "A cluster of melioidosis cases from an endemic region is clonal and is linked to the water supply using molecular typing of Burkholderia pseudomallei isolates". The American Journal of Tropical Medicine and Hygiene.
- (December 1999). "Acute melioidosis outbreak in Western Australia". Epidemiology and Infection.
- (February 2014). "Melioidosis caused by Burkholderia pseudomallei in drinking water, Thailand, 2012". Emerging Infectious Diseases.
- (March 2011). "Molecular phylogeny of Burkholderia pseudomallei from a remote region of Papua New Guinea". PLOS ONE.
- (February 2022). "Melioidosis of the central nervous system; the impact of the bimABm allele on patient presentation and outcome". Clinical Infectious Diseases.
- (August 2010). "Defining the true sensitivity of culture for the diagnosis of melioidosis using Bayesian latent class models". PLOS ONE.
- (June 2006). "An improved selective and differential medium for the isolation of Burkholderia pseudomallei from clinical specimens". Diagnostic Microbiology and Infectious Disease.
- (September 2012). "Development of a multiplex PCR assay for rapid identification of Burkholderia pseudomallei, Burkholderia thailandensis, Burkholderia mallei and Burkholderia cepacia complex". Journal of Microbiological Methods.
- (October 2003). "Use of 16S rRNA gene sequencing for rapid identification and differentiation of Burkholderia pseudomallei and B. mallei". Journal of Clinical Microbiology.
- (March 2022). "Reliable detection of Burkholderia pseudomallei using multiple cross displacement amplification label-based biosensor". BMC Microbiology.
- (2013). "Potential immunogenic polypeptides of Burkholderia pseudomallei identified by shotgun expression library and evaluation of their efficacy for serodiagnosis of melioidosis". International Journal of Medical Sciences.
- (November 2007). "Accuracy of Burkholderia pseudomallei identification using the API 20NE system and a latex agglutination test". Journal of Clinical Microbiology.
- (June 2015). "Laboratory diagnosis of melioidosis: past, present and future". Experimental Biology and Medicine.
- (December 2019). "Clinical Epidemiology of 7126 Melioidosis Patients in Thailand and the Implications for a National Notifiable Diseases Surveillance System". Open Forum Infectious Diseases.
- (October 2020). "Imported melioidosis in the United Kingdom: Increasing incidence but continued under-reporting". Journal of Clinical Microbiology.
- Centers for Disease Control and Prevention. (2009). "Biosafety in Microbiological and Biomedical Laboratories". National Institutes of Health.
- (March 2017). "Burkholderia pseudomallei: Challenges for the Clinical Microbiology Laboratory-a Response from the Front Line". Journal of Clinical Microbiology.
- (November 2003). "The effect of free chlorine on Burkholderia pseudomallei in potable water". Water Research.
- (August 2013). "Melioidosis from contaminated bore water and successful UV sterilization". The American Journal of Tropical Medicine and Hygiene.
- (2013). "Activities of daily living associated with acquisition of melioidosis in northeast Thailand: a matched case-control study". PLOS Neglected Tropical Diseases.
- (June 2021). "Effectiveness of a multifaceted prevention programme for melioidosis in diabetics (PREMEL): A stepped-wedge cluster-randomised controlled trial". PLOS Neglected Tropical Diseases.
- (September 2018). "Antibiotic Prophylaxis for Melioidosis in Patients Receiving Hemodialysis in the Tropics? One Size Does Not Fit All". The American Journal of Tropical Medicine and Hygiene.
- (December 2012). "Workshop on treatment of and postexposure prophylaxis for Burkholderia pseudomallei and B. mallei Infection, 2010". Emerging Infectious Diseases.
- (January 2014). "Burkholderia pseudomallei isolates from Sarawak, Malaysian Borneo, are predominantly susceptible to aminoglycosides and macrolides". Antimicrobial Agents and Chemotherapy.
- (September 1989). "Halving of mortality of severe melioidosis by ceftazidime". Lancet.
- (September 1989). "Interactions in vitro between agents used to treat melioidosis". The Journal of Antimicrobial Chemotherapy.
- Currie BJ. (2015). "Mandell, Douglas, and Bennett's Principles and Practice of Infectious Diseases". Elsevier.
- (February 2008). "Consensus guidelines for dosing of amoxicillin-clavulanate in melioidosis". The American Journal of Tropical Medicine and Hygiene.
- (November 1994). "Ceftazidime vs. amoxicillin/clavulanate in the treatment of severe melioidosis". Clinical Infectious Diseases.
- (September 2020). "2020 Review and revision of the 2015 Darwin melioidosis treatment guideline; paradigm drift not shift". PLOS Neglected Tropical Diseases.
- (April 2014). "Treatment and prophylaxis of melioidosis". International Journal of Antimicrobial Agents.
- (March 2002). "The role of cefoperazone-sulbactam for treatment of severe melioidosis". Clinical Infectious Diseases.
- (December 2021). "A Comparison Between 12 Versus 20 Weeks of Trimethoprim-sulfamethoxazole as Oral Eradication Treatment for Melioidosis: An Open-label, Pragmatic, Multicenter, Non-inferiority, Randomized Controlled Trial". Clinical Infectious Diseases.
- (October 2014). "Trimethoprim/sulfamethoxazole resistance in Burkholderia pseudomallei". International Journal of Antimicrobial Agents.
- (May 2015). "Trimethoprim/sulfamethoxazole resistance in clinical isolates of Burkholderia pseudomallei from Thailand". International Journal of Antimicrobial Agents.
- (June 2021). "Interpreting Burkholderia pseudomallei disc diffusion susceptibility test results by the EUCAST method". Clinical Microbiology and Infection.
- (January 2005). "Mycotic aneurysm due to Burkholderia pseudomallei infection: case reports and literature review". Clinical Infectious Diseases.
- (January 2018). "Prostatic Abscess due to ''Burkholderia pseudomallei'': Facilitating Diagnosis to Optimize Management". The American Journal of Tropical Medicine and Hygiene.
- (April 2009). "Melioidotic prostatic abscess in Pahang". Singapore Medical Journal.
- (August 2009). "Prostatic abscess due to Burkholderia pseudomallei: 81 cases from a 19-year prospective melioidosis study". The Journal of Urology.
- (May 2015). "Programmed death ligand 1 on Burkholderia pseudomallei-infected human polymorphonuclear neutrophils impairs T cell functions". Journal of Immunology.
- "Melioidosis Locally Endemic in Areas of the Mississippi Gulf Coast after Burkholderia pseudomallei Isolated in Soil and Water and Linked to Two Cases – Mississippi, 2020 and 2022". CDC.
This article was imported from Wikipedia and is available under the Creative Commons Attribution-ShareAlike 4.0 License. Content has been adapted to SurfDoc format. Original contributors can be found on the article history page.
Ask Mako anything about Melioidosis — get instant answers, deeper analysis, and related topics.
Research with MakoFree with your Surf account
Create a free account to save articles, ask Mako questions, and organize your research.
Sign up freeThis content may have been generated or modified by AI. CloudSurf Software LLC is not responsible for the accuracy, completeness, or reliability of AI-generated content. Always verify important information from primary sources.
Report