From Surf Wiki (app.surf) — the open knowledge base
Left bundle branch block

| Field | Value |
|---|---|
| name | Left bundle branch block |
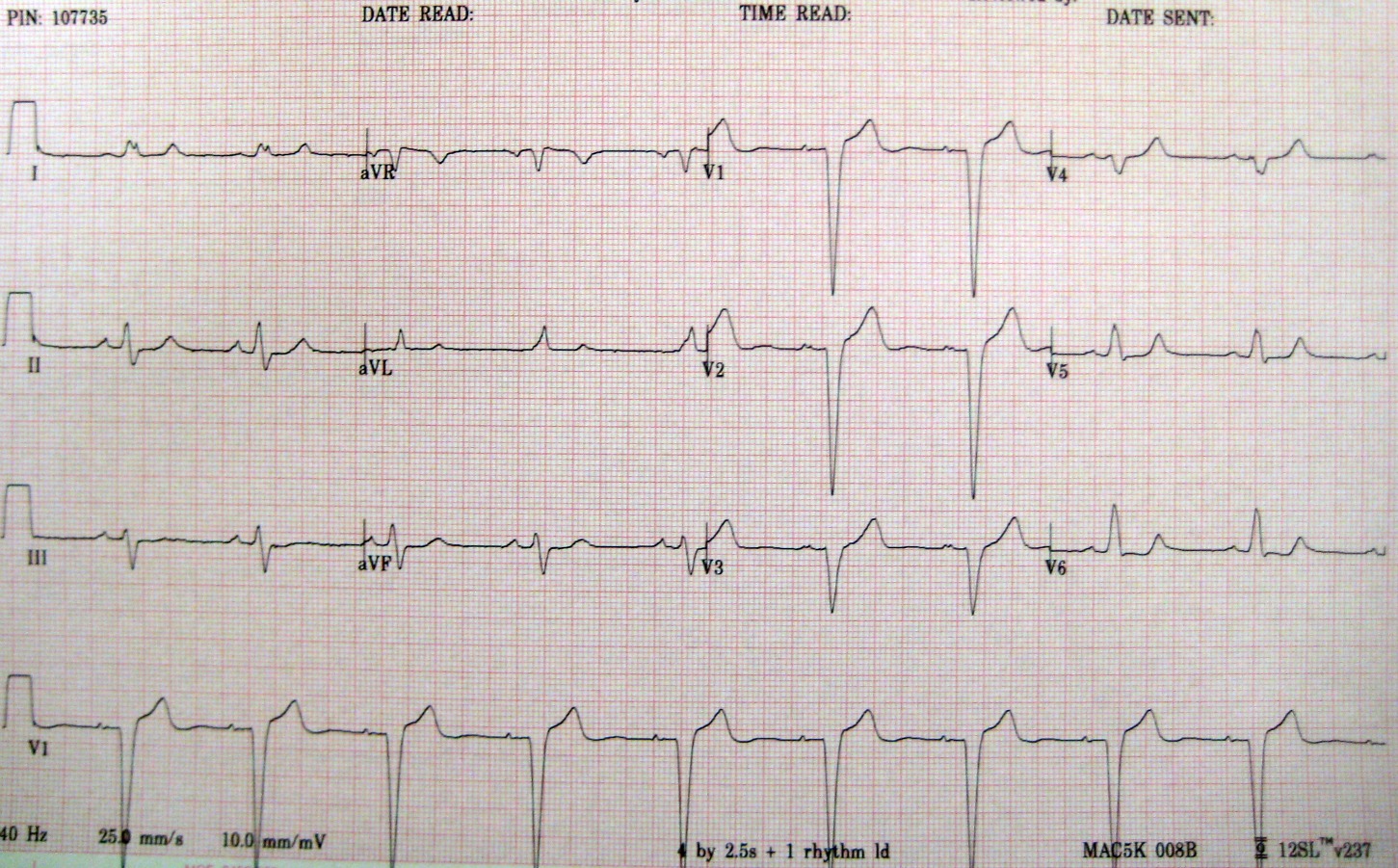
| image | Left bundle branch block ECG characteristics.svg |
| caption | ECG characteristics of a typical LBBB showing wide QRS complexes with abnormal morphology in leads V1 and V6. |
| field | Cardiology, Emergency Medicine |
Left bundle branch block (LBBB) is a conduction abnormality in the heart that can be seen on an electrocardiogram (ECG). In this condition, activation of the left ventricle of the heart is delayed, which causes the left ventricle to contract later than the right ventricle.
Causes
Among the causes of LBBB are:
- Aortic stenosis
- Dilated cardiomyopathy
- Acute myocardial infarction
- Extensive coronary artery disease
- Primary disease of the cardiac electrical conduction system
- Long standing hypertension leading to aortic root dilatation and subsequent aortic regurgitation
- Lyme disease
Mechanisms
Slow or absent conduction through the left bundle branch means that it takes longer than normal for the left ventricle to fully depolarise. This can be due to a damaged bundle branch that is completely unable to conduct, but may represent intact conduction that is slower than normal. LBBB may be fixed, present at all times, but may be intermittent for example occurring only during rapid heart rates. This may be due to the bundle having a longer refractory period than usual.
Diagnosis
There are also partial blocks of the left bundle branch: "left anterior fascicular block" (LAFB) and a "left posterior fascicular block" (LPFB). This refers to the block after the bifurcation of the left bundle branch.
Diagnostic consequences
The presence of LBBB results in that electrocardiography (ECG) cannot be used to diagnose left ventricular hypertrophy or Q wave infarction, because LBBB in itself results in a widened QRS complex and changes in the ST segment consistent with ischemia or injury.
BARCELONA Criteria
Given the difficulty diagnosing an acute myocardial infarction (AMI) in patients with pre-existing LBBB, a multicenter retrospective cohort study was done to help improve diagnosis of AMI in this patient population. Sgarbossa criteria and its Modified Criteria have historically been used to determine AMI in patients with LBB, but the clinical utility has a high specificity (90%) with a low sensitivity (36%).
Two new approaches to the ECG were elaborated to improve the diagnostic sensitivity of ECG in patients with LBBB and suspected AMI. First, since any ST deviation concordant with the QRS should be regarded as abnormal, it was hypothesized that not only concordant ST elevation but also concordant ST depression might be a sign of AMI. The Sgarbossa rule of concordant ST depression in leads V1 to V3 was then extended to include any other lead to, in theory, cover the electrocardiographic projection of acute ischemia in different myocardial regions. Second, the presence of an appreciable (≥1 mm or 0.1 mV) discordant ST deviation in low‐voltage QRS complexes was considered as a positive criterion for AMI. This criterion was included because in the absence of ischemia, these complexes usually show isoelectric ST‐segment potentials.
The results of the study resulted in the development of the BARCELONA algorithm. Under these criteria, an ECG is positive for an AMI in the presence of LBBB if any of the following criteria are present:
- ST deviation ≥1 mm (0.1 mV) concordant with QRS polarity in any ECG lead, thus including either:
- ST depression ≥1 mm (0.1 mV) concordant with QRS polarity, in any ECG lead.
- ST elevation ≥1 mm (0.1 mV) concordant with QRS polarity, in any ECG lead (Sgarbossa score 5).
- ST deviation ≥1 mm (0.1 mV) discordant with QRS polarity, in any lead with max (R|S) voltage ≤6 mm (0.6 mV).
The BARCELONA algorithm attained the highest sensitivity (95%), significantly higher (P
Treatment
- Patients with LBBB require complete cardiac evaluation, and those with LBBB and syncope or near-syncope may require a pacemaker.
- Some patients with LBBB, a markedly prolonged QRS (usually 150 ms), and systolic heart failure may benefit from a biventricular pacemaker, which allows for better synchrony of heart contractions.
References
References
- "Conduction Blocks". Kansas City University of Medicine & Biosciences.
- "Bundle branch block: Symptoms and causes". Mayo Clinic.
- (2007). "Twelve-lead electrocardiography: theory and interpretation". Springer.
- (March 2009). "AHA/ACCF/HRS recommendations for the standardization and interpretation of the electrocardiogram: part III: intraventricular conduction disturbances: a scientific statement from the American Heart Association Electrocardiography and Arrhythmias Committee, Council on Clinical Cardiology; the American College of Cardiology Foundation; and the Heart Rhythm Society. Endorsed by the International Society for Computerized Electrocardiology". Journal of the American College of Cardiology.
- {{Cite GPnotebook. x20050921122910832459. More detailed information about left anterior fascicular block
- (13 May 2014). "Electrocardiography > Left Bundle Branch Block (LBBB)". [[Southern Illinois University School of Medicine]].
- (July 2020). "New Electrocardiographic Algorithm for the Diagnosis of Acute Myocardial Infarction in Patients With Left Bundle Branch Block". Journal of the American Heart Association.
- (February 2012). "Indications for cardiac resynchronization therapy: 2011 update from the Heart Failure Society of America Guideline Committee". Journal of Cardiac Failure.
This article was imported from Wikipedia and is available under the Creative Commons Attribution-ShareAlike 4.0 License. Content has been adapted to SurfDoc format. Original contributors can be found on the article history page.
Ask Mako anything about Left bundle branch block — get instant answers, deeper analysis, and related topics.
Research with MakoFree with your Surf account
Create a free account to save articles, ask Mako questions, and organize your research.
Sign up freeThis content may have been generated or modified by AI. CloudSurf Software LLC is not responsible for the accuracy, completeness, or reliability of AI-generated content. Always verify important information from primary sources.
Report