From Surf Wiki (app.surf) — the open knowledge base
Hypoadrenocorticism in dogs

| Field | Value |
|---|---|
| name | Hypoadrenocorticism in dogs |
| synonyms | adrenal insufficiency, hypocortisolism |
| field | Veterinary medicine |
Hypoadrenocorticism in dogs, or, as it is known in people, Addison's disease, is an endocrine system disorder that occurs when the adrenal glands fail to produce enough hormones for normal function. The adrenal glands secrete glucocorticoids such as cortisol and mineralocorticoids such as aldosterone; when proper amounts of these are not produced, the metabolic and electrolyte balance is upset. Mineralocorticoids control the amount of potassium, sodium, and water in the body. Hypoadrenocorticism is fatal if left untreated.
The most common cause of inadequate adrenal production is idiopathic adrenocortical atrophy. All causes for hypoadrenocorticism are not yet known. The usual causes are genetic, often related to autoimmune disorders, where the body attacks and kill its own tissue ("immune mediated destruction"). including failure of the pituitary gland to secrete ACTH, the hormone which stimulates the adrenal production of cortisol.
Hypoadrenocorticism is more frequent in dogs than in humans; in fact, it may occur one hundred times more often in the canine population. It mostly affects young to middle-aged female dogs,
Signs and symptoms
The most common clinical manifestations are related to mental status and gastrointestinal function; they include lethargy, anorexia, vomiting, weight loss, and weakness. Additional findings may include dehydration, bradycardia, weak femoral pulses, abdominal pain, lack of appetite, tremors or shaking, muscle weakness, low body temperature, collapse, and pain in the hindquarters. Polyuria and polydipsia, diarrhea, and shivering are occasionally reported.
Hypoglycemia can also be present, and initially may be confused with a seizure disorder or an insulin-secreting pancreatic tumor (insulinoma). Hypoadrenocorticism may also be misdiagnosed as food poisoning, parvovirus enteritis, gastric volvulus, or spinal/joint problems, earning this disease nicknames like "the Great Mimic" and "the Great Imitator". It is possible not to see any signs of the disease until 90% of the adrenal cortex is no longer functioning.
Addisonian crisis
If hyponatremia (low sodium) and hyperkalemia (high potassium) are severe, the resulting hypovolemia, prerenal azotemia, and cardiac arrhythmias may result in an Addisonian crisis. In severe cases, the patient may be presented in shock and moribund. Addisonian crisis must be differentiated from other life-threatening disorders such as diabetic ketoacidosis, necrotizing pancreatitis, and septic peritonitis.
Causes
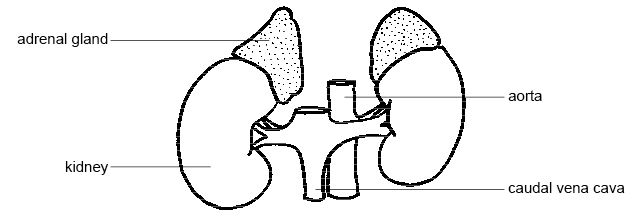
The adrenal glands are located above the kidneys. The adrenal outer layer, or cortex, has three layers; each produces a specific type of steroid.
| Layer | Type of steroid produced | Example |
|---|---|---|
| Zona glomerulosa | Mineralocorticoids | aldosterone |
| Zona fasciculata | Glucocorticoids | cortisol |
| Zona reticularis | Sex steroids (androgens) |
Primary
Primary adrenocortical insufficiency is the more common form of hypoadrenocorticism. All layers of the adrenal gland stop functioning; the problem is with the adrenal gland. This causes a deficiency of both mineralocorticoid and glucocorticoid secretion. Most cases are classified as idiopathic, although immune-mediated adrenocortical destruction is a likely cause. Bilateral destruction of the adrenal cortex by neoplasia (e.g. lymphosarcoma), granulomatous disease, or arterial thrombosis can also cause primary adrenocortical insufficiency. The destruction is progressive, although variable in rate, ultimately leading to complete loss of adrenocorotical function. A partial deficiency syndrome may occur initially, with signs manifested only during times of stress (e.g., boarding, travel, surgery).
Secondary

In secondary hypoadrenocorticism the problem is not in the adrenal gland but in the pituitary gland. Usually, the anterior portion of the pituitary gland produces a hormone, adrenocorticotropic hormone (ACTH), that signals the zona fasciculata and zona reticularis to produce their steroids. When the pituitary is unable to produce ACTH, these zones stop production of their hormones. The zona glomerulosa is not controlled by ACTH, and remains able to produce a normal amount of mineralocorticoids. A dog with secondary hypoadrenocorticism only needs to have medication to replace the glucocorticoid steroid cortisol. One dog in every 42 diagnosed with hypoadrenocorticism has the secondary form of the disease where mineralocorticoid production remains intact.
Secondary adrenocortical insufficiency involves only a deficiency of glucocorticoid secretion. Destructive lesions (e.g. neoplasia, inflammation) in the pituitary gland or hypothalamus and chronic administration of exogenous glucocorticoids or megestrol acetate (cats) are the most common causes.
Drug induced
Drug induced (iatrogenic) hypoadrenocorticism is caused during abrupt cessation of a steroid medication. During steroid treatment, the adrenal glands do not function fully. The body senses the levels of the exogenous steroids in the system and therefore does not signal for additional production. The usual protocol for stopping steroid medications is not to eliminate them suddenly, but to withdraw from them gradually in a "tapering off" process, which allows the production to adjust to normal. If steroids are abruptly withdrawn, the dormant adrenal glands may not able to reactivate, and the body will need to have its adrenal glucocorticoid hormones replaced by medication.
Diagnosis
Hypoadrenocorticism is often tentatively diagnosed on the basis of history, physical findings, clinical pathology, and, for primary adrenal insufficiency, characteristic electrolyte abnormalities.
- Clinical pathology - Abnormalities may be identified on hematology, biochemistry and urinalysis. Elevated concentrations of potassium (hyperkalemia), and low sodium and chloride values (hyponatremia and hypochloremia) are the classic electrolyte alterations. The sodium/potassium ratio often is
- ECG - The severity of the ECG abnormalities correlates with the severity of the hyperkalemia. Therefore, the ECG can be used to identify and estimate the severity of hyperkalemia and to monitor changes in serum potassium during therapy.
- Diagnostic imaging - Abdominal ultrasound may reveal small adrenal glands, suggesting adrenocortical atrophy. However, finding normal-sized adrenal glands does not rule out hypoadrenocorticism. Rarely, megaesophagus is evident on radiographs.
- ACTH stimulation test - Confirmation requires evaluation of an ACTH stimulation test. Baseline plasma cortisol and urine cortisol/Cr ratios are unreliable for confirming the diagnosis. One major diagnostic criterion is abnormally decreased post-ACTH plasma cortisol. Normal plasma cortisol after ACTH stimulation rules out adrenal insufficiency. The only accurate test for hypoadrenocorticism is an ACTH stimulation test; however, any administration of a steroid other than dexamethasone will invalidate this test. Carry out test by:
- Measuring serum cortisol before and after administration of ACTH gel or synthetic ACTH
- Normal dogs generally have post stimulation cortisol levels 10 ug/dl.
- Post stimulation levels
- Measuring serum cortisol before and after administration of ACTH gel or synthetic ACTH
The ACTH stimulation test does not distinguish between primary and secondary hypoadrenocorticism, or adrenocortical destruction caused by mitotane overdose. Differentiation between primary and secondary hypoadrenocorticism can be made by periodically measuring serum electrolytes, baseline endogenous ACTH, or possibly serum or plasma aldosterone during the ACTH stimulation test. While most corticosteroid drugs will invalidate the results of an ACTH test, dexamethasone may be used in the event of an Addison's emergency without fear of compromising the results of the test.
In general, hypoadrenocorticism is underdiagnosed in dogs, and one must have a clinical suspicion of it as an underlying disorder for many presenting complaints. Females are overrepresented (~70% of cases), and the disease often appears in middle age (four to seven years), although any age or gender may be affected. Dogs with hypoadrenocorticism may also have one of several autoimmune disorders. Because it is an endocrine disorder, they may also have neuropathy and some endocrine-related eye diseases.
Addisonian crisis
If deterioration of the adrenal glands progresses far enough, a dog may experience an Addisonian crisis, an acute episode during which potassium levels increase (hyperkalemia), disrupting normal functions of the heart. Some 35% of canine Addison's cases are diagnosed as the result of an Addisonian crisis. It is a medical emergency.
Whipworms
Dogs with infected with the whipworm Trichuris trichiura can exhibit low sodium and high potassium values, as is seen in hypoadrenocorticism; however, their ACTH values are normal.
Pacific Rim
Breeds that began in the Pacific Rim, among them Akitas and Shiba Inus, tend to have higher potassium values in laboratory test, and elevated levels are not abnormal. Dogs who do not have hypoadrenocorticism have normal values on ACTH tests.
Treatment
Aggressiveness of therapy depends on the clinical status of the patient and the nature of the insufficiency (glucocorticoid, mineralocorticoid, or both). Many dogs and cats with primary adrenal insufficiency are presented in Addisonian crisis and require immediate, aggressive therapy. In contrast, secondary insufficiency often has a chronic course.
Hypoadrenocorticism is treated with oral daily administration of fludrocortisone (trade name Florinef) or a monthly injection of desoxycorticosterone pivalate, DOCP (Percorten-V or Zycortal) and daily prednisone or prednisolone. One drug is needed to supplement mineralcortidoids and the other to supplement corticosteroids. This effectively replaces what the adrenal cortex is failing to produce. Routine blood work is necessary in the initial stages until a maintenance dose is established. Most of the medications used in the therapy of hypoadrenocorticism cause excessive thirst and urination. It is absolutely vital to provide fresh drinking water for a canine with this disorder.
If the owner knows about an upcoming stressful situation (shows, traveling etc.), the animals generally need an increased dose of prednisone (2-4 times maintenance) to help deal with the added stress. Avoidance of stress is important for dogs with hypoadrenocorticism. Physical illness also stresses the body and may mean that the medication(s) need to be adjusted during this time. Most dogs with hypoadrenocorticism have an excellent prognosis after proper stabilization and treatment.
Addisonian crisis
Treatment is directed towards (1) correcting hypotension, hypovolemia, electrolyte imbalances, and metabolic acidosis; (2) improving vascular integrity, and (3) providing an immediate source of glucocorticoids. Rapid correction of hypovolemia is the first priority.
Restoring blood volume is vital to correcting hypotension, hypovolemia, and addressing electrolyte and metabolic imbalances. This is achieved by the rapid administration of fluids. This helps to correct hyponatremia, restore perfusion to organs, and reduce hyperkalemia through increased GFR and dilution effects. Further treatment of hyperkalemia is addressed if necessary. Often, the fluid therapy can sufficiently address hyperkalemia, but in the presence of significant cardiac abnormalities, the addition of calcium gluconate may be necessary in addition to glucose, insulin, or bicarb to promote intracellular shift of potassium.
Most patients show dramatic improvement within 24 to 48 hours of appropriate fluid and glucocorticoid therapy. Over the ensuing 2 to 4 days, a gradual transition from IV fluids to oral water and food is undertaken, and maintenance mineralocorticoid and glucocorticoid therapy is initiated. Failure to make this transition smoothly should raise suspicion of insufficient glucocorticoid supplementation, concurrent endocrinopathy (e.g. hypothyroidism), or concurrent illness (especially renal damage).
It is important that after the crisis is corrected that the patient is put on a maintenance therapy of corticosteroids and mineralocorticoids.
Epidemiology
Hypoadrenocorticism is typically a disease of young to middle-aged female dogs, although Standard Poodles and Bearded Collies of both sexes are prone to the condition.
Hypoadrenocorticism is an inherited disease in the following breeds (and therefore a higher proportion of dogs within these breeds are affected, compared to other breeds):
- Bearded Collie
- Nova Scotia Duck Tolling Retriever
- Portuguese Water Dog
- Standard Poodle
Some breeds are at increased risk of hypoadrenocorticism:
- Airedale Terrier
- Basset Hound
- Bearded Collie
- Great Dane
- Rottweiler
- Springer Spaniels: English Springer Spaniel and Welsh Springer Spaniel
- Saint Bernard
- Soft-Coated Wheaten Terrier
- West Highland white terrier
Some breeds have a reduced risk of hypoadrenocorticism:
- Boxer
- Cocker Spaniel
- Golden Retriever
- Pit Bull Terrier
- Lhasa Apso
- Yorkshire Terrier
History
The first case of hypoadrenocorticism in dogs was recorded in 1953, over 100 years after it was described in humans by Thomas Addison.
References
References
- "Adrenal Steroids". School of Veterinary Medicine-Colorado State University.
- "Mineralocorticoids". School of Veterinary Medicine-Colorado State University.
- Stoeppler, Melissa Conrad. "What Are Electrolytes?". MedicineNet.
- "Addison's Disease (Hypoadrenocorticism) in Dogs". Drs. Foster & Smith.
- Hardy, RM. "Hypoadrenal gland disease". WB Saunders.
- Ettinger, Feldman. "Textbook of Veterinary Internal Medicine 5th ed".
- Schaer, Michael. (2005). "Acute Adrenocortical Insufficiency". 30th World Congress of the World Small Animal Veterinary Association.
- Kelch, WJ. (June 1998). "Canine hypoadrenocorticism (Addison's Disease)". The Compendium.
- Gough, Alex (2007). Differential diagnosis in Small Animal Medicine. Blackwell Publishing: Carlton, Victoria.
- (2008). "Adrenal Cortex". Merck Veterinary Manual.
- Nelson and Couto (2005). Manual of Small Animal [[Internal medicine. Internal Medicine]]. 2nd Edition. Elsevier Mosby: St. Louis, Missouri. p.503-507
- "Overview of Adrenal Histology". School of Veterinary Medicine-Colorado State University.
- Maddison, Jill. (2009). "Corticosteroids: Friend or Foe?". Proceedings of the 34th World Congress of the World Small Animal Veterinary Association.
- (November 2014). "Demystifying Tests for Hyperadrenocorticism". Clinicians' Brief.
- (2008). "Use of a low-dose ACTH stimulation test for diagnosis of hypoadrenocorticism in dogs.". Journal of Veterinary Internal Medicine.
- (November 1, 2008). "Consider ACTH stimulation test when you suspect canine hyperadrenocorticism". dvm360.com.
- "ACTH Stimulation Test". Idexx.
- "Guide to Endocrinology".
- Brooks, Wendy C.. "Addison's Disease (Hypoadrenocorticism)". Veterinary Partner.
- "Dog Days of Science". National Institutes of Health.
- Plummer, Caryn E.. (December 2007). "Ocular Manifestations of Endocrine Disease". Compendium.
- "Addison's Disease". New Hope Animal Hospital.
- Nussey, SS.. (2001). "Endocrinology-an Integrated Approach-Aldosterone". National Institutes of Health (US).
- (2010). "Canine hypoadrenocorticism: part II". The Canadian Veterinary Journal.
- Durkan, Samuel. (January 2008). "Endocrine Emergencies". DVM 360.
- "What Is Addison's Disease?". MarVista Vet.
- "Fludrocortisone Acetate". National Institutes of Health.
- Brooks, Wendy C.. "Fludrocortisone Acetate (Florinef)". Veterinary Partner.
- "About Percorten-V-Treatment for Canine Addison's Disease". Novartis Animal Health.
- "Percorten-V Product Information". Novartis Animal Health.
- Church, David B.. (2009). "Management of Hypoadrenocorticism". Proceedings of the 34th World Congress of the World Small Animal Veterinary Association.
- "Zycortal". Dechra.
- (2008). "Hypoadrenocorticism". The Merck Veterinary Manual.
- Spielman, Bari. "Hypoadrenocorticism (Addison's Disease) in Dogs". PetPlace.com.
- "Adrenal Insufficiency and Addison's Disease". National Endocrine and Metabolic Diseases Information Service.
- "Addison's Disease". Southpaws Veterinary Center.
- (February 2005). "Canine Hypoadrenocorticism: Pathogenesis and Clinical Features". VetFolio.
- (2014). "Canine and feline endocrinology". Saunders Elsevier.
- (2010). "Canine hypoadrenocorticism: part I". The Canadian Veterinary Journal.
- (29 April 1989). "Addison's disease in the dog.". The Veterinary Record.
This article was imported from Wikipedia and is available under the Creative Commons Attribution-ShareAlike 4.0 License. Content has been adapted to SurfDoc format. Original contributors can be found on the article history page.
Ask Mako anything about Hypoadrenocorticism in dogs — get instant answers, deeper analysis, and related topics.
Research with MakoFree with your Surf account
Create a free account to save articles, ask Mako questions, and organize your research.
Sign up freeThis content may have been generated or modified by AI. CloudSurf Software LLC is not responsible for the accuracy, completeness, or reliability of AI-generated content. Always verify important information from primary sources.
Report