From Surf Wiki (app.surf) — the open knowledge base
Endometrial cancer
Uterine cancer that is located in tissues lining the uterus
Uterine cancer that is located in tissues lining the uterus
| Field | Value |
|---|---|
| name | Endometrial cancer. |
| synonyms | Uterine cancer |
| image | File:Blausen 0348 EndometrialCancer.png |
| caption | The location and development of endometrial cancer |
| alt | A diagram of the location and development of endometrial cancer |
| field | Oncology, gynecology |
| symptoms | Vaginal bleeding, pain with urination or sexual intercourse, pelvic pain |
| onset | After menopause |
| risks | Obesity, excessive estrogen exposure, high blood pressure, diabetes, family history |
| diagnosis | Endometrial biopsy |
| treatment | Abdominal hysterectomy, radiation therapy, chemotherapy, hormone therapy |
| prognosis | Five-year survival rate ~80% (US) |
| frequency | 3.8 million (total affected in 2015) |
| deaths | 89,900 (2015) |
Endometrial cancer is a cancer that arises from the endometrium (the lining of the uterus or womb). It is the result of the abnormal growth of cells that can invade or spread to other parts of the body. The first sign is most often vaginal bleeding not associated with a menstrual period.
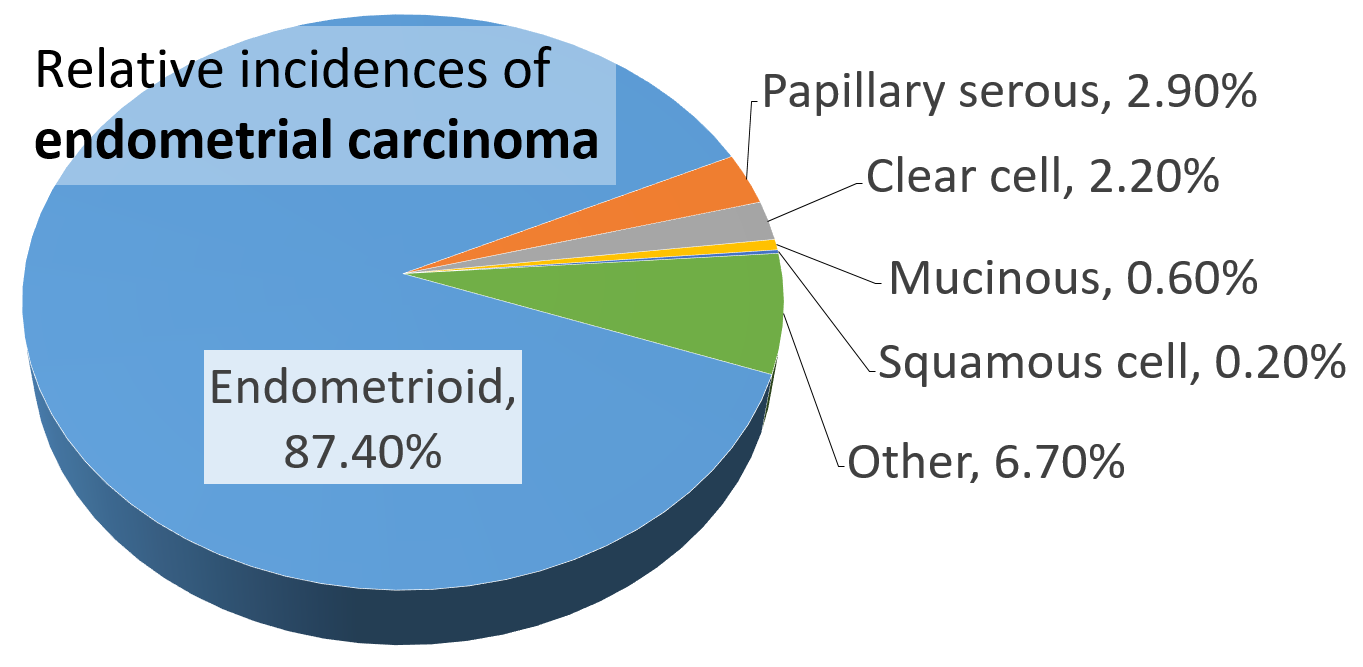
Approximately 40% of cases are related to obesity. Endometrial cancer is also associated with excessive estrogen exposure, high blood pressure and diabetes. The most frequent type of endometrial cancer is endometrioid carcinoma, which accounts for more than 80% of cases. Endometrial cancer is commonly diagnosed by endometrial biopsy or by taking samples during a procedure known as dilation and curettage. Regular screening in those at normal risk is not called for.
The leading treatment option for endometrial cancer is abdominal hysterectomy (the total removal by surgery of the uterus), together with removal of the Fallopian tubes and ovaries on both sides, called a bilateral salpingo-oophorectomy.
In 2012, endometrial cancers newly occurred in 320,000 women and caused 76,000 deaths. This makes it the third most common cause of death in cancers which only affect women, behind ovarian and cervical cancer.
Signs and symptoms
Vaginal bleeding or spotting in women after menopause occurs in 90% of endometrial cancer. Bleeding is quite common with adenocarcinoma, occurring in two-thirds of all cases. Abnormal menstrual cycles or extremely long, heavy, or frequent episodes of bleeding in women before menopause may also be a sign of endometrial cancer.
Symptoms other than bleeding are not common. Other symptoms include thin white or clear vaginal discharge in postmenopausal women.
Risk factors
Risk factors for endometrial cancer include obesity, insulin resistance and diabetes mellitus, breast cancer, use of tamoxifen, never having had a child, late menopause, high levels of estrogen, and increasing age. Immigration studies (migration studies), which examine the change in cancer risk in populations moving between countries with different rates of cancer, show that there is some environmental component to endometrial cancer. These environmental risk factors are not well characterized.
Hormones
Most of the risk factors for endometrial cancer involve high levels of estrogens. An estimated 40% of cases are thought to be related to obesity. In obesity, the excess of adipose tissue increases conversion of androstenedione into estrone, an estrogen. Higher levels of estrone in the blood causes less or no ovulation and exposes the endometrium continuously to high levels of estrogens. Obesity also causes less estrogen to be removed from the blood. Polycystic ovary syndrome (PCOS), which also causes irregular or no ovulation, is associated with higher rates of endometrial cancer for the same reasons as obesity. Specifically, obesity, type II diabetes, and insulin resistance are risk factors for Type I endometrial cancer. Obesity increases the risk for endometrial cancer by 300–400%.
Estrogen replacement therapy during menopause when not balanced (or "opposed") with progestin is another risk factor. Higher doses or longer periods of estrogen therapy have higher risks of endometrial cancer. Unopposed estrogen raises an individual's risk of endometrial cancer by 2–10 fold, depending on weight and length of therapy. In trans men who take testosterone and have not had a hysterectomy, the conversion of testosterone into estrogen via androstenedione may lead to a higher risk of endometrial cancer. Higher circulating testosterone levels in women have also been identified as an independent endometrial cancer risk factor.
Genetics

Genetic disorders can also cause endometrial cancer. Overall, hereditary causes contribute to 2–10% of endometrial cancer cases. Carcinogenesis in Lynch syndrome comes from a mutation in MLH1 or MLH2: genes that participate in the process of mismatch repair, which allows a cell to correct mistakes in the DNA. Other genes mutated in Lynch syndrome include MSH2, MSH6, and PMS2, which are also mismatch repair genes. Women with Lynch syndrome represent 2–3% of endometrial cancer cases; some sources place this as high as 5%. Depending on the gene mutation, women with Lynch syndrome have different risks of endometrial cancer. With MLH1 mutations, the risk is 54%; with MSH2, 21%; and with MSH6, 16%.
Women with a family history of endometrial cancer are at higher risk. Two genes most commonly associated with some other women's cancers, BRCA1 and BRCA2, do not cause endometrial cancer. There is an apparent link with these genes. It is attributable to the use of tamoxifen, a drug that itself can cause endometrial cancer, in breast and ovarian cancers. The inherited genetic condition Cowden syndrome can also cause endometrial cancer. Women with this disorder have a 5–10% lifetime risk of developing endometrial cancer, compared to the 2–3% risk for unaffected women.
Common genetic variation has also been found to affect endometrial cancer risk in large-scale genome-wide association studies. Sixteen genomic regions have been associated with endometrial cancer and the common variants explain up to 7% of the familial relative risk.
Other health problems
Some therapies for other forms of cancer increase the lifetime risk of endometrial cancer, which is a baseline 2–3%. A one to two-year course of tamoxifen approximately doubles the risk of endometrial cancer, and a five-year course of therapy quadruples that risk. Raloxifene, a similar drug, did not raise the risk of endometrial cancer. as is having had previous radiotherapy to the pelvis. Specifically, ovarian granulosa cell tumors and thecomas are tumors associated with endometrial cancer.
Low immune function has also been implicated in endometrial cancer.
Protective factors
Smoking and the use of progestin are both protective against endometrial cancer. Smoking protects by altering the metabolism of estrogen and promoting weight loss and early menopause. This protective effect lasts long after smoking is stopped. Progestin is present in the combined oral contraceptive pill and the hormonal intrauterine device (IUD). Combined oral contraceptives reduce risk more the longer they are taken: by 56% after four years, 67% after eight years, and 72% after twelve years. This risk reduction continues for at least fifteen years after contraceptive use has been stopped. Mendelian randomization analyses have established potential protective factors such as LDL cholesterol, later age of menarche and sex hormone binding globulin.
Pathophysiology
| Gene mutated | Mutation type | Type I prevalence | Type II prevalence |
|---|---|---|---|
| ARID1A | point mutation | 40% | unknown |
| CTNNB1 | point mutation | 14–44% | unknown |
| FGFR2 | point mutation | 16% | unknown |
| KRAS | point mutation | 10–20% | unknown |
| PIK3R1 | point mutation | 43% | unknown |
| TP53 | point mutation | 10–20% | 90% |
| PTEN | point mutation | 37–61% | unknown |
| MLH1 | epigenetic silencing | 30% | unknown |
| RASSF1A | epigenetic silencing | 48% | unknown |
| SPRY2 | epigenetic silencing | 20% | unknown |
| PPP2R1A | point mutation | unknown | 17–41% |
| CDH1 | loss of heterozygosity | unknown | 80–90% |
| CDKN2A | loss of heterozygosity or | ||
| epigenetic silencing | 20% | 40% | |
| PIK3CA (oncogene) | point mutation or amplification | 24–39% | 20–30% |
| PIK3R1 (oncogene) | point mutation | unknown | 12% |
| STK15 (oncogene) | amplification | unknown | 60% |
| CCNE1 (oncogene) | amplification | unknown | 55% |
| ERBB2 (oncogene) | amplification | unknown | 30% |
| CCND1 (oncogene) | amplification | unknown | 26% |
|} Endometrial cancer forms when there are errors in normal endometrial cell growth. Usually, when cells grow old or get damaged, they die, and new cells take their place. Cancer starts when new cells form unneeded, and old or damaged cells do not die as they should. The buildup of extra cells often forms a mass of tissue called a growth or tumor. These abnormal cancer cells have many genetic abnormalities that cause them to grow excessively.
In 10–20% of endometrial cancers, mostly Grade 3 (the highest histologic grade), mutations are found in a tumor suppressor gene, commonly p53 or PTEN. In 20% of endometrial hyperplasias and 50% of endometrioid cancers, PTEN has a loss-of-function mutation or a null mutation, making it less effective or completely ineffective. Loss of PTEN function leads to up-regulation of the PI3k/Akt/mTOR pathway, which causes cell growth. The p53 pathway can either be suppressed or highly activated in endometrial cancer. When a mutant version of p53 is overexpressed, the cancer tends to be particularly aggressive. P53 mutations and chromosome instability are associated with serous carcinomas, which tend to resemble ovarian and Fallopian carcinomas. Serous carcinomas are thought to develop from endometrial intraepithelial carcinoma.

PTEN and p27 loss of function mutations are associated with a good prognosis, particularly in obese women. The Her2/neu oncogene, which indicates a poor prognosis, is expressed in 20% of endometrioid and serous carcinomas. CTNNB1 (beta-catenin; a transcription gene) mutations are found in 14–44% of endometrial cancers and may indicate a good prognosis, but the data is unclear. SPOP is another tumor suppressor gene found to be mutated in some cases of endometrial cancer: 9% of clear cell endometrial carcinomas and 8% of serous endometrial carcinomas have mutations in this gene.
Type I and Type II cancers (explained below) tend to have different mutations involved. ARID1A, which often carries a point mutation in Type I endometrial cancer, is also mutated in 26% of clear cell carcinomas of the endometrium and 18% of serous carcinomas. Epigenetic silencing and point mutations of several genes are commonly found in Type I endometrial cancer. Mutations in tumor suppressor genes are common in Type II endometrial cancer. PIK3CA is commonly mutated in both Type I and Type II cancers. In women with Lynch syndrome-associated endometrial cancer, microsatellite instability is common.
Development of an endometrial hyperplasia (overgrowth of endometrial cells) is a significant risk factor because hyperplasias can and often do develop into adenocarcinoma, though cancer can develop without the presence of a hyperplasia. An atypical hyperplasia is one with visible abnormalities in the nuclei. Pre-cancerous endometrial hyperplasias are also referred to as endometrial intraepithelial neoplasia. Mutations in the KRAS gene can cause endometrial hyperplasia and therefore Type I endometrial cancer.
Diagnosis
Diagnosis of endometrial cancer is made first by a physical examination, endometrial biopsy, or dilation and curettage (removal of endometrial tissue; D&C). This tissue is then examined histologically for characteristics of cancer. If cancer is found, medical imaging may be done to see whether the cancer has spread or invaded tissues like the myometrium (the muscular wall of the womb) or the uterine cervix. A study from 2024 indicates that transvaginal ultrasound provides diagnostic performance comparable to magnetic resonance imaging regarding the myometrial infiltration assessment. However, magnetic resonance imaging showed significantly better specificity in low-grade endometrial cancer.
Examination
![An ultrasound image showing an endometrial fluid accumulation (darker area) in a [[postmenopausal]] uterus, a finding that is highly suspicious for endometrial cancer](https://upload.wikimedia.org/wikipedia/commons/b/bd/Endometrial_fluid_accumulation,_postmenopausal.jpg)

Routine screening of asymptomatic people is not indicated since the disease is highly curable in its early, symptomatic stages. Instead, women, particularly menopausal women, should be aware of the symptoms and risk factors of endometrial cancer. A cervical screening test, such as a Pap smear, is not a useful diagnostic tool for endometrial cancer because the smear will be normal 50% of the time.
Women with Lynch syndrome should begin to have annual biopsy screening at the age of 35. Some women with Lynch syndrome elect to have a prophylactic hysterectomy and salpingo-oophorectomy to greatly reduce the risk of endometrial and ovarian cancer.
Transvaginal ultrasound to examine the endometrial thickness in women with postmenopausal bleeding is increasingly being used to aid in the diagnosis of endometrial cancer in the United States. In the United Kingdom, both an endometrial biopsy and a transvaginal ultrasound used in conjunction are the standard of care for diagnosing endometrial cancer. They can also be used to investigate extrapelvic disease. An MRI can be of some use in determining if the cancer has spread to the cervix or if it is an endocervical adenocarcinoma. MRI is also useful for examining the nearby lymph nodes.
Dilation and curettage or an endometrial biopsy are used to obtain a tissue sample for histological examination. Endometrial biopsy is the less invasive option, but it may not give conclusive results every time. Hysteroscopy only shows the gross anatomy of the endometrium, which is often not indicative of cancer and is, therefore, not used unless in conjunction with a biopsy. Hysteroscopy can be used to confirm a diagnosis of cancer. New evidence shows that D&C has a higher false negative rate than endometrial biopsy.
Before treatment is begun, several other investigations are recommended. These include a chest x-ray, liver function tests, kidney function tests, and a test for levels of CA-125, a tumor marker that can be elevated in endometrial cancer.
Classification
Endometrial cancers may be tumors derived from epithelial cells (carcinomas), mixed epithelial and mesenchymal tumors (carcinosarcomas), or mesenchymal tumors.
Traditional classification of endometrial carcinomas is based either on clinical and endocrine features (Type I and Type II) or histopathological characteristics (endometrioid, serous, and clear-cell). Some tumors are difficult to classify and have features overlapping more than one category. High-grade endometrioid tumors, in particular, tend to have both type I and type II features.
Carcinoma
The vast majority of endometrial cancers are carcinomas (usually adenocarcinomas), meaning that they originate from the single layer of epithelial cells that line the endometrium and form the endometrial glands. There are many microscopic subtypes of endometrial carcinoma, but they are broadly organized into two categories, Type I and Type II, based on clinical features and pathogenesis. The two subtypes are genetically distinct.
Type I endometrial carcinomas occur most commonly before and around the time of menopause. In the United States, they are more common in white women, particularly those with a history of endometrial hyperplasia. Type I endometrial cancers are often low-grade, minimally invasive into the underlying uterine wall (myometrium), estrogen-dependent, and have a good outcome with treatment. Type I carcinomas represent 75–90% of endometrial cancer.
Type II endometrial carcinomas usually occur in older, post-menopausal people. In the United States, they are more common in black women and are not associated with increased exposure to estrogen or a history of endometrial hyperplasia. Type II endometrial cancers are often high-grade, with deep invasion into the underlying uterine wall (myometrium), are of the serous or clear cell type, and carry a poorer prognosis. They can appear to be epithelial ovarian cancer on evaluation of symptoms. They tend to present later than Type I tumors and are more aggressive, with a greater risk of relapse and/or metastasis.
Endometrioid adenocarcinoma
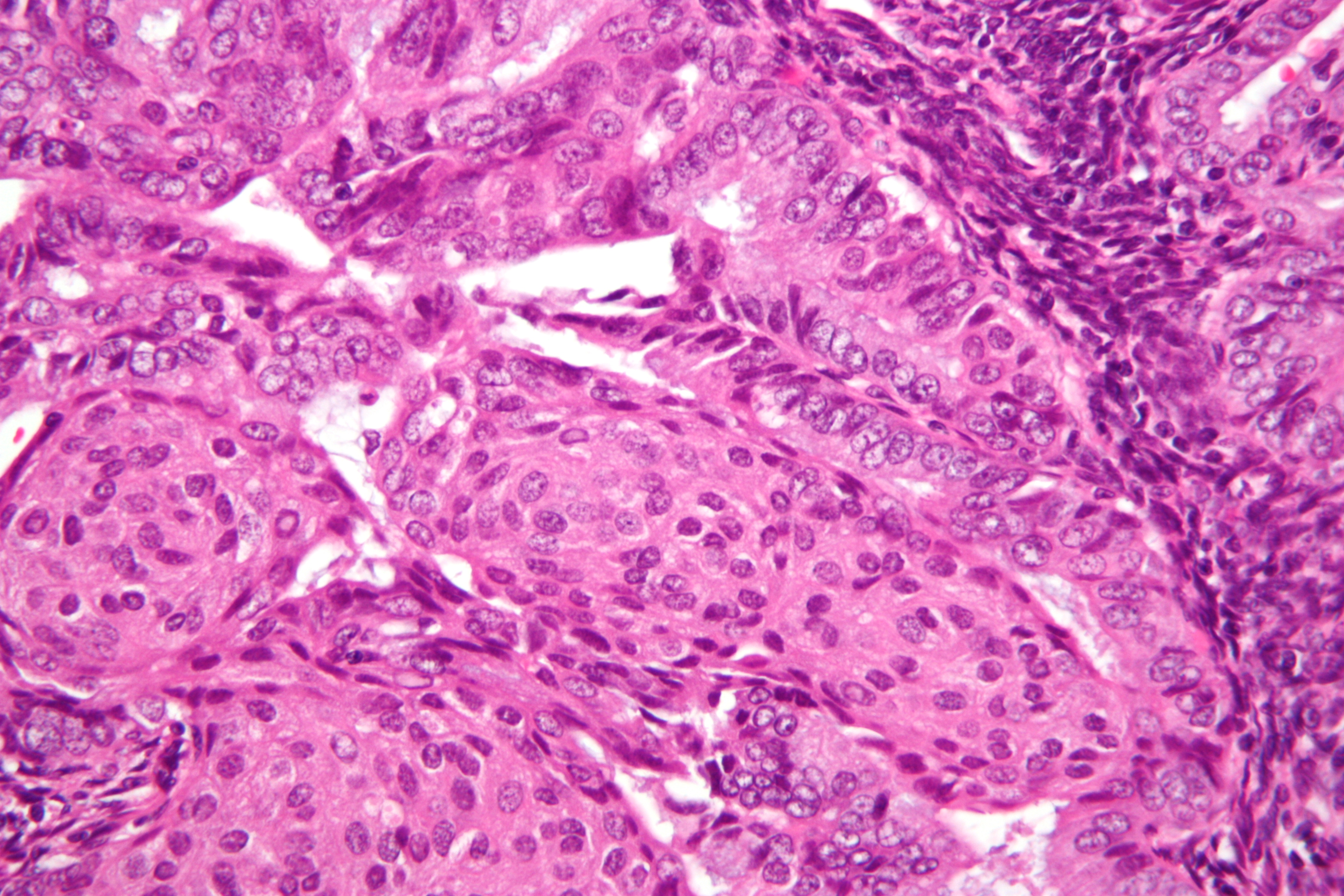
In endometrioid adenocarcinoma, the cancer cells grow in patterns reminiscent of normal endometrium, with many new glands formed from columnar epithelium with some abnormal nuclei. Low-grade endometrioid adenocarcinomas have well-differentiated cells, have not invaded the myometrium, and are seen alongside endometrial hyperplasia. The tumor's glands form very close together, without the stromal tissue that normally separates them. Higher-grade endometrioid adenocarcinomas have less well-differentiated cells, have more solid sheets of tumor cells no longer organized into glands, and are associated with an atrophied endometrium. There are several subtypes of endometrioid adenocarcinoma with similar prognoses, including villoglandular, secretory, and ciliated cell variants. There is also a subtype characterized by squamous differentiation. Some endometrioid adenocarcinomas have foci of mucinous carcinoma.
The genetic mutations most commonly associated with endometrioid adenocarcinoma are in the genes PTEN, a tumor suppressor; PIK3CA, a kinase; KRAS, a GTPase that functions in signal transduction; and CTNNB1, involved in adhesion and cell signaling. The CTNNB1 (beta-catenin) gene is most commonly mutated in the squamous subtype of endometrioid adenocarcinoma.
Serous carcinoma
Serous carcinoma is a Type II endometrial tumor that makes up 5–10% of diagnosed endometrial cancer and is common in postmenopausal women with atrophied endometrium and black women. Serous endometrial carcinoma is aggressive and often invades the myometrium and metastasizes within the peritoneum (seen as omental caking) or the lymphatic system. Histologically, it appears with many atypical nuclei, papillary structures, and, in contrast to endometrioid adenocarcinomas, rounded cells instead of columnar cells. Roughly 30% of endometrial serous carcinomas also have psammoma bodies. Serous carcinomas spread differently than most other endometrial cancers; they can spread outside the uterus without invading the myometrium.
The genetic mutations seen in serous carcinoma are chromosomal instability and mutations in TP53, an important tumor suppressor gene.
Clear cell carcinoma
Clear cell carcinoma is a Type II endometrial tumor that makes up less than 5% of diagnosed endometrial cancer. Like serous cell carcinoma, it is usually aggressive and carries a poor prognosis. Histologically, it is characterized by the features common to all clear cells: the eponymous clear cytoplasm when H&E stained and visible, distinct cell membranes. The p53 cell signaling system is not active in endometrial clear cell carcinoma. This form of endometrial cancer is more common in postmenopausal women.
Mucinous carcinoma
Mucinous carcinomas are a rare form of endometrial cancer, making up less than 1–2% of all diagnosed endometrial cancers. Mucinous endometrial carcinomas are most often stage I and grade I, giving them a good prognosis. They typically have well-differentiated columnar cells organized into glands with the characteristic mucin in the cytoplasm. Mucinous carcinomas must be differentiated from cervical adenocarcinoma.
Mixed or undifferentiated carcinoma
Mixed carcinomas are those that have both Type I and Type II cells, with one making up at least 10% of the tumor.
Undifferentiated endometrial carcinomas make up less than 1–2% of diagnosed endometrial cancers. They have a worse prognosis than grade III tumors. Histologically, these tumors show sheets of identical epithelial cells with no identifiable pattern.
Other carcinomas
Non-metastatic squamous cell carcinoma and transitional cell carcinoma are very rare in the endometrium. Squamous cell carcinoma of the endometrium has a poor prognosis. Primary transitional cell carcinomas of the endometrium are even more rare; 16 cases had been reported . Its pathophysiology and treatments have not been characterized. Histologically, TCCE resembles endometrioid carcinoma and is distinct from other transitional cell carcinomas.
Sarcoma
Main article: Endometrial stromal sarcoma
In contrast to endometrial carcinomas, the uncommon endometrial stromal sarcomas are cancers that originate in the non-glandular connective tissue of the endometrium. They are generally non-aggressive and, if they recur, can take decades. Metastases to the lungs and pelvic or peritoneal cavities are the most frequent. The prognosis for low-grade endometrial stromal sarcoma is good, with 60–90% five-year survival. High-grade undifferentiated endometrial sarcoma (HGUS) has a worse prognosis, with high rates of recurrence and 25% five-year survival. HGUS prognosis is dictated by whether or not the cancer has invaded the arteries and veins. Without vascular invasion, the five-year survival is 83%; it drops to 17% when vascular invasion is observed. Stage I ESS has the best prognosis, with a five-year survival rate of 98% and a ten-year survival rate of 89%. ESS makes up 0.2% of uterine cancers.
Metastasis
Endometrial cancer frequently metastasizes to the ovaries and Fallopian tubes Endometrial cancer metastasizes to the lungs 20–25% of the time, more than any other gynecologic cancer.
Histopathology

There is a three-tiered system for histologically classifying endometrial cancers, ranging from cancers with well-differentiated cells (grade I), to very poorly-differentiated cells (grade III). Grade I cancers are the least aggressive and have the best prognosis, while grade III tumors are the most aggressive and likely to recur. Grade II cancers are intermediate between grades I and III in terms of cell differentiation and aggressiveness of disease. There is also a separate "nuclear grade" system, where grade 1 tumors have inconspicuous cell nuclei, whereas grade 3 tumors have highly atypical nuclei.
The histopathology of endometrial cancers is highly diverse. The most common finding is a well-differentiated endometrioid adenocarcinoma, which is composed of numerous, small, crowded glands with varying degrees of nuclear atypia, mitotic activity, and stratification. This often appears on a background of endometrial hyperplasia. Frank adenocarcinoma may be distinguished from atypical hyperplasia by the finding of clear stromal invasion, or "back-to-back" glands, which represent nondestructive replacement of the endometrial stroma by the cancer. With progression of the disease, the myometrium is infiltrated. File:Endometrioid adenocarcinoma of the uterus FIGO grade III.jpg|A stage III endometrioid adenocarcinoma that has invaded the myometrium File:Metastatic endometrial carcinoma (3944215367).jpg|Metastatic endometrial cancer seen in a removed lung File:Histopathology of FIGO (architectural) grade 1 endometrial adenocarcinoma.png|Grade 1: ≤5% solid non-glandular, non-squamous growth. File:FIGO grade 2 endometrial adenocarcinoma.jpg|Grade 2: 5% and ≤50% solid non-glandular, non-squamous growth. File:FIGO grade 3 endometrial adenocarcinoma.jpg|Grade 3: 50% solid non-glandular, non-squamous growth. File:Histopathology of endometrioid cancer, grade 1, nuclear grade 1.jpg|Nuclear grade 1: Oval, mildly enlarged nucleus with evenly distributed chromatin. File:Histopathology of endometrioid cancer, grade 1, nuclear grade 2.jpg|Nuclear grade 2: Intermediate features. File:Endometrial endometrioid adenocarcinoma, nuclear and architectural grade 3.jpg|Nuclear grade 3: Markedly enlarged and pleomorphic nuclei, with coarse chromatin and distinct nucleoli. File:Endometrial endometrioid carcinoma with squamous differentiation and keratin granulomas, high magnification.jpg|Squamous growth seen as necrotic "ghost cells" of keratinocytes at right in image, leaving pink keratin.
Staging
Endometrial carcinoma is surgically staged using the FIGO cancer staging system. The 2009 FIGO staging system is commonly used. There is an updated 2023 FIGO staging system, but it is not yet universally adopted. The 2009 FIGO staging system is as follows:
| Stage | Description |
|---|---|
| IA | Tumor is confined to the uterus with less than half myometrial invasion |
| IB | Tumor is confined to the uterus with more than half myometrial invasion |
| II | Tumor involves the uterus and the cervical stroma |
| IIIA | Tumor invades serosa or adnexa |
| IIIB | Vaginal and/or parametrial involvement |
| IIIC1 | Pelvic lymph node involvement |
| IIIC2 | Para-aortic lymph node involvement, with or without pelvic node involvement |
| IVA | Tumor invades bladder mucosa and/or bowel mucosa |
| IVB | Distant metastases including abdominal metastases and/or inguinal lymph nodes |

_of_endometrial_adenocarcinoma_in_a_lymph_node.png)
Myometrial invasion and involvement of the pelvic and para-aortic lymph nodes are the most commonly seen patterns of spread. A Stage 0 is sometimes included; in this case, it is referred to as "carcinoma in situ". In 26% of presumably early-stage cancers, intraoperative staging revealed pelvic and distant metastases, making comprehensive surgical staging necessary. File:Diagram showing stage 1A and 1B cancer of the womb CRUK 196.svg|alt=A diagram of stage IA and IB endometrial cancer|Stage IA and IB endometrial cancer File:Diagram showing stage 2 cancer of the womb CRUK 206.svg|alt=A diagram of stage II endometrial cancer|Stage II endometrial cancer File:Diagram showing stage 3A to 3C cancer of the womb CRUK 224.svg|alt=A diagram of stage III endometrial cancer|Stage III endometrial cancer File:Diagram showing stage 4A and 4B cancer of the womb CRUK 234.svg|alt=A diagram of stage IV endometrial cancer|Stage IV endometrial cancer
Management
Surgery

The initial treatment for endometrial cancer is surgery; 90% of women with endometrial cancer are treated with some form of surgery. Surgical treatment typically consists of hysterectomy including a bilateral salpingo-oophorectomy, which is the removal of the uterus, both ovaries, and the Fallopian tubes. Lymphadenectomy, or removal of pelvic and para-aortic lymph nodes, is performed for tumors of histologic grade II or above. Lymphadenectomy is routinely performed for all stages of endometrial cancer in the United States, but in the United Kingdom, the lymph nodes are typically only removed with disease of stage II or greater. Women who undergo lymphadenectomy are more likely to experience systemic morbidity related to surgery or lymphoedema/lymphocyst formation. In stage III and IV cancers, cytoreductive surgery is the norm, and a biopsy of the omentum may also be included. Removal of the uterus via the abdomen is recommended over removal of the uterus via the vagina because it allows examining and obtaining washings of the abdominal cavity to detect any further evidence of cancer. Staging of the cancer is done during the surgery.
The few contraindications to surgery include inoperable tumor, massive obesity, a particularly high-risk operation, or a desire to preserve fertility. Uterine perforation may occur during a D&C or an endometrial biopsy. Side effects of surgery to remove endometrial cancer can specifically include sexual dysfunction, temporary incontinence, and lymphedema, along with more common side effects of any surgery, including constipation.
Add-on therapy
There are many possible additional therapies. Surgery can be followed by radiation therapy and/or chemotherapy in cases of high-risk or high-grade cancers. This is called adjuvant therapy.
Chemotherapy
Adjuvant chemotherapy is a recent innovation, consisting of some combination of paclitaxel (or other taxanes like docetaxel), doxorubicin (and other anthracyclines), and platins (particularly cisplatin and carboplatin). Adjuvant chemotherapy has been found to increase survival in stage III and IV cancer more than added radiotherapy. Mutations in mismatch repair genes, like those found in Lynch syndrome, can lead to resistance against platins, meaning that chemotherapy with platins is ineffective in people with these mutations. Side effects of chemotherapy are common. These include hair loss, low neutrophil levels in the blood, and gastrointestinal problems.
In cases where surgery is not indicated, palliative chemotherapy is an option; higher-dose chemotherapy is associated with longer survival. Palliative chemotherapy, particularly using capecitabine and gemcitabine, is also often used to treat recurrent endometrial cancer.
Low-certainty evidence suggests that in women with recurrent endometrial cancer who have had chemotherapy, receiving drugs that inhibit the mTOR pathway may reduce the risk of disease worsening compared to having more chemotherapy or hormonal therapy. However, mTOR inhibitors may increase the chance of experiencing digestive tract ulcers.
Radiotherapy
Adjuvant radiotherapy is commonly used in early-stage (stage I or II) endometrial cancer. It can be delivered through vaginal brachytherapy (VBT), which is becoming the preferred route due to its reduced toxicity, or external beam radiotherapy (EBRT). Brachytherapy involves placing a radiation source in the organ affected; in the case of endometrial cancer a radiation source is placed directly in the vagina. External beam radiotherapy involves a beam of radiation aimed at the affected area from outside the body. VBT is used to treat any remaining cancer solely in the vagina, whereas EBRT can be used to treat remaining cancer elsewhere in the pelvis following surgery. However, the benefits of adjuvant radiotherapy are controversial. Though EBRT significantly reduces the rate of relapse in the pelvis, overall survival and metastasis rates are not improved. VBT provides a better quality of life than EBRT.
Radiotherapy can also be used before surgery in certain cases. When pre-operative imaging or clinical evaluation shows tumor invading the cervix, radiation can be given before a total hysterectomy is performed. Brachytherapy and EBRT can also be used, singly or in combination, when there is a contraindication for hysterectomy. Both delivery methods of radiotherapy are associated with side effects, particularly in the gastrointestinal tract.
Hormonal therapy
Hormonal therapy is only beneficial in certain types of endometrial cancer. It was once thought to be beneficial in most cases. About 25% of metastatic endometrioid cancers show a response to progestins. Also, endometrial stromal sarcomas can be treated with hormonal agents, including tamoxifen, hydroxyprogesterone caproate, letrozole, megestrol acetate, and medroxyprogesterone. Preliminary research and clinical trials have shown these treatments to have a high rate of response even in metastatic disease.
In 2010, hormonal therapy was of unclear effect in those with advanced or recurrent endometrial cancer. There is insufficient evidence to inform women considering hormone replacement therapy after treatment for endometrial cancer.
Targeted therapy
Dostarlimab has been approved by the FDA for therapy of endometrial cancer with specific biomarker
Monitoring
The tumor marker CA-125 is frequently elevated in endometrial cancer and can be used to monitor response to treatment, particularly in serous cell cancer or advanced disease. Periodic MRIs or CT scans may be recommended in advanced disease and women with a history of endometrial cancer should receive more frequent pelvic examinations for the five years following treatment. Examinations conducted every three to four months are recommended for the first two years following treatment, and every six months for the next three years.
Women with endometrial cancer should not have routine surveillance imaging to monitor the cancer unless new symptoms appear or tumor markers begin rising. Imaging without these indications is discouraged because it is unlikely to detect a recurrence or improve survival and because it has its costs and side effects. If a recurrence is suspected, PET/CT scanning is recommended.
Prognosis
Survival rates
| Stage | 5-year survival rate |
|---|---|
| I-A | 88% |
| I-B | 75% |
| II | 69% |
| III-A | 58% |
| III-B | 50% |
| III-C | 47% |
| IV-A | 17% |
| IV-B | 15% |
The five-year survival rate for endometrial adenocarcinoma following appropriate treatment is 80%. More than 70% of women diagnosed have FIGO stage I cancer, which has the best prognosis. Stage III and especially Stage IV cancers have a worse prognosis, but these are relatively rare, occurring in only 13% of cases. The median survival time for stage III–IV endometrial cancer is nine to ten months. Older age indicates a worse prognosis. In the United States, white women have a higher survival rate than black women, who tend to develop more aggressive forms of the disease by the time of their diagnosis. Tumors with high progesterone receptor expression have a good prognosis compared to tumors with low progesterone receptor expression; 93% of women with high progesterone receptor disease survived to three years, compared with 36% of women with low progesterone receptor disease. with other obesity-related health problems also being common. Following diagnosis, quality of life is also positively associated with a healthy lifestyle (no obesity, high-quality diet, physical activity).
Recurrence rates
Main article: Cancer recurrence
Recurrence of early-stage endometrial cancer ranges from 3% to 17%, depending on primary and adjuvant treatment. Most recurrences (75–80%) occur outside of the pelvis, and most occur within two to three years of treatment—64% within two years and 87% within three years.
Higher-staged cancers are more likely to recur, as are those that have invaded the myometrium or cervix or that have metastasized into the lymphatic system. Papillary serous carcinoma, clear cell carcinoma, and endometrioid carcinoma are the subtypes at the highest risk of recurrence. High-grade histological subtypes are also at elevated risk for recurrence.
The most common site of recurrence is in the vagina; Radiation therapy (VBT and EBRT) for a local vaginal recurrence has a 50% five-year survival rate. Pelvic recurrences are treated with surgery and radiation, and abdominal recurrences are treated with radiation and, if possible, chemotherapy.
Epidemiology
, approximately 320,000 women are diagnosed with endometrial cancer worldwide each year and 76,000 die, making it the sixth most common cancer in women. It is more common in developed countries, where the lifetime risk of endometrial cancer in women is 1.6%, compared to 0.6% in developing countries. It occurs in 12.9 out of 100,000 women annually in developed countries.
In the United States, endometrial cancer is the most frequently diagnosed gynecologic cancer and, in women, the fourth most common cancer overall, representing 6% of all cancer cases in women. In that country, it was estimated that 52,630 women were diagnosed yearly and 8,590 would die from the disease. Northern Europe, Eastern Europe, and North America have the highest rates of endometrial cancer, whereas Africa and West Asia have the lowest rates. Asia saw 41% of the world's endometrial cancer diagnoses in 2012, whereas Northern Europe, Eastern Europe, and North America together comprised 48% of diagnoses. Unlike most cancers, the number of new cases has risen in recent years, including an increase of over 40% in the United Kingdom between 1993 and 2013. Some of this rise may be due to the increase in obesity rates in developed countries, increasing life expectancies, and lower birth rates.
Endometrial cancer appears most frequently during perimenopause (the period just before, just after, and during menopause), between the ages of 50 and 65; overall, 75% of endometrial cancer occurs after menopause. Women younger than 40 make up 5% of endometrial cancer cases and 10–15% of cases occur in women under 50 years of age. This age group is at risk for developing ovarian cancer at the same time. The worldwide median age of diagnosis is 63 years of age; in the United States, the average age of diagnosis is 60 years of age. White American women are at higher risk for endometrial cancer than black American women, with a 2.88% and 1.69% lifetime risk, respectively. Japanese-American women and American Latina women have lower rates, and Native Hawaiian women have higher rates.
Research
There are several experimental therapies for endometrial cancer under research, including immunologic, hormonal, and chemotherapeutic treatments. Trastuzumab (Herceptin), an antibody against the Her2 protein, has been used in cancers known to be positive for the Her2/neu oncogene, but research is still underway. Immunologic therapies are also under investigation, particularly in uterine papillary serous carcinoma.
Cancers can be analyzed using genetic techniques (including DNA sequencing and immunohistochemistry) to determine if certain therapies specific to mutated genes can be used to treat it. PARP inhibitors are used to treat endometrial cancer with PTEN mutations, specifically, mutations that lower the expression of PTEN. The PARP inhibitor shown to be active against endometrial cancer is olaparib. Research has been ongoing in this area as of the 2010s.
Research is ongoing on the use of metformin, a diabetes medication, in obese women with endometrial cancer before surgery. Early research has shown it to be effective in slowing the rate of cancer cell proliferation. Preliminary research has shown that preoperative metformin administration can reduce the expression of tumor markers. Long-term use of metformin has not been shown to have a preventative effect against developing cancer, but it may improve overall survival.
Temsirolimus, an mTOR inhibitor, is under investigation as a potential treatment. Research shows that mTOR inhibitors may be particularly effective for cancers with mutations in PTEN. Ridaforolimus (deforolimus) is also being researched as a treatment for people who have previously had chemotherapy. Preliminary research has been promising, and a stage II trial for ridaforolimus was completed by 2013. There has also been research on combined ridaforolimus/progestin treatments for recurrent endometrial cancer. Bevacizumab and tyrosine kinase inhibitors, which inhibit angiogenesis, are being researched as potential treatments for endometrial cancers with high levels of vascular endothelial growth factor. Ixabepilone is being researched as a possible chemotherapy for advanced or recurrent endometrial cancer. Treatments for rare high-grade undifferentiated endometrial sarcoma are being researched, as there is no established standard of care yet for this disease. Chemotherapies being researched include doxorubicin and ifosfamide.
There is also research in progress on more genes and biomarkers that may be linked to endometrial cancer. The protective effect of combined oral contraceptives and the IUD is being investigated. Preliminary research has shown that the levonorgestrel IUD placed for a year, combined with six monthly injections of gonadotropin-releasing hormone, can stop or reverse the progress of endometrial cancer in young women, specifically complex atypical hyperplasia; however, the results have been inconclusive. An experimental drug that combines a hormone with doxorubicin is also under investigation for greater efficacy in cancers with hormone receptors. Hormone therapy that is effective in treating breast cancer, including the use of aromatase inhibitors, is also being investigated for use in endometrial cancer. One such drug is anastrozole, which is currently being researched in hormone-positive recurrences after chemotherapy. Research into hormonal treatments for endometrial stromal sarcomas is ongoing as well. It includes trials of drugs like mifepristone, a progestin antagonist, and aminoglutethimide and letrozole, two aromatase inhibitors.
Research continues into the best imaging method for detecting and staging endometrial cancer. As current diagnostic methods are invasive and inaccurate, researchers are looking into new ways to catch endometrial cancer, especially in its early stages. A study found that using a technique involving infrared light on simple blood test samples detected uterine cancer with high accuracy (87%) and could detect precancerous growths in all cases. In surgery, research has shown that complete pelvic lymphadenectomy along with hysterectomy in stage 1 endometrial cancer does not improve survival and increases the risk of negative side effects, including lymphedema. Other research is exploring the potential of identifying the sentinel lymph nodes for biopsy by injecting the tumor with dye that shines under infrared light. Intensity modulated radiation therapy is currently under investigation and already used in some centers for application in endometrial cancer to reduce side effects from traditional radiotherapy. Its risk of recurrence has not yet been quantified. Research on hyperbaric oxygen therapy to reduce side effects is also ongoing. The results of the PORTEC 3 trial assessing combining adjuvant radiotherapy with chemotherapy were awaited in late 2014.
There is not enough evidence to determine if people with endometrial cancer benefit from additional behavioural and lifestyle interventions that are aimed at losing excess weight.
History and culture
Endometrial cancer is not widely known by the general populace despite its frequency. There is low awareness of the symptoms, which can lead to later diagnosis and worse survival.
References
References
- (October 2016). "Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990-2015: a systematic analysis for the Global Burden of Disease Study 2015". Lancet.
- (October 2016). "Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980-2015: a systematic analysis for the Global Burden of Disease Study 2015". Lancet.
- (22 April 2014). "General Information About Endometrial Cancer". National Cancer Institute.
- (2007-09-17). "Defining Cancer". National Cancer Institute.
- (April 2012). "Adjuvant radiotherapy for stage I endometrial cancer". The Cochrane Database of Systematic Reviews.
- International Agency for Research on Cancer. (2014). "World Cancer Report 2014". [[World Health Organization]].
- (2012). "Williams Gynecology". [[McGraw-Hill]].
- "SEER Stat Fact Sheets: Endometrial Cancer". [[National Cancer Institute]].
- (2012). "Williams Gynecology". [[McGraw-Hill]].
- "Uterine Cancer - Cancer Stat Facts".
- (2022). "Endometrial cancer". The Lancet.
- (2021-12-09). "Endometrial cancer". Nature Reviews Disease Primers.
- (May 2014). "Adjuvant chemotherapy for advanced endometrial cancer". The Cochrane Database of Systematic Reviews.
- (2012). "Williams Gynecology". [[McGraw-Hill]].
- (July 2022). "Impact of metabolic syndrome on the risk of endometrial cancer and the role of lifestyle in prevention". Bosnian Journal of Basic Medical Sciences.
- (August 2012). "Chemotherapy for advanced, recurrent or metastatic endometrial carcinoma". The Cochrane Database of Systematic Reviews.
- (December 2011). "Committee Opinion no. 512: health care for transgender individuals". Obstetrics and Gynecology.
- (May 2023). "Multi-trait genome-wide association study identifies a novel endometrial cancer risk locus that associates with testosterone levels". iScience.
- (June 2016). "Five endometrial cancer risk loci identified through genome-wide association analysis". Nature Genetics.
- (August 2018). "Identification of nine new susceptibility loci for endometrial cancer". Nature Communications.
- (2013). "Comprehensive Gynecology". [[Mosby (publisher).
- (January 2015). "Sedentary time and its association with risk for disease incidence, mortality, and hospitalization in adults: a systematic review and meta-analysis". Annals of Internal Medicine.
- (2012). "Williams Gynecology". [[McGraw-Hill]].
- (March 2022). "10 Years of GWAS discovery in endometrial cancer: Aetiology, function and translation". eBioMedicine.
- (January 2019). "Interpretation of P53 Immunohistochemistry in Endometrial Carcinomas: Toward Increased Reproducibility". International Journal of Gynecological Pathology.
- (2012-01-01). "Comprehensive Gynecology". [[Mosby (publisher).
- (September 2014). "The emerging role of speckle-type POZ protein (SPOP) in cancer development". Drug Discovery Today.
- (2012). "Williams Gynecology". [[McGraw-Hill]].
- Madár, I.; Szabó, A.; Vleskó, G.; Hegyi, P.; Ács, N.; Fehérvári, P.; Kói, T.; Kálovics, E.; Szabó, G. Diagnostic Accuracy of Transvaginal Ultrasound and Magnetic Resonance Imaging for the Detection of Myometrial Infiltration in Endometrial Cancer: A Systematic Review and Meta-Analysis. Cancers 2024, 16, 907. https://doi.org/10.3390/cancers16050907
- (2012). "Williams Gynecology". [[McGraw-Hill]].
- (June 2014). "Classification of endometrial carcinoma: more than two types". The Lancet. Oncology.
- (January 2009). "Non-endometrioid adenocarcinoma of the uterine corpus: a review of selected histological subtypes". Cancer Control.
- (2012). "Williams Gynecology". [[McGraw-Hill]].
- (September 2011). "Endometrial cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up". Annals of Oncology.
- (October 2011). "Adjuvant chemotherapy for endometrial cancer after hysterectomy". The Cochrane Database of Systematic Reviews.
- (November 2008). "Transitional cell carcinoma of the endometrium and endometrial carcinoma with transitional cell differentiation: a clinicopathologic study of 5 cases and review of the literature". Human Pathology.
- (October 2006). "Transitional cell carcinoma of the endometrium: a case report and review of the literature". International Journal of Gynecological Pathology.
- (2012). "Uterine sarcomas: histology and its implications on therapy". American Society of Clinical Oncology Educational Book. American Society of Clinical Oncology. Annual Meeting.
- (January 2010). "Uterine sarcomas: a review". Gynecologic Oncology.
- (2012). "Williams Gynecology". [[McGraw-Hill]].
- (2012). "Williams Gynecology". [[McGraw-Hill]].
- Nofech-Mozes S, Ismiil N, Dubé V, Saad RS, Ghorab Z, Grin A. (2012). "Interobserver agreement for endometrial cancer characteristics evaluated on biopsy material.". Obstet Gynecol Int.
- (2019). "Endometrial Carcinoma Diagnosis". International Journal of Gynecological Pathology.
- Nofech-Mozes S, Ismiil N, Dubé V, Saad RS, Ghorab Z, Grin A. (2012). "Interobserver agreement for endometrial cancer characteristics evaluated on biopsy material.". Obstet Gynecol Int.
- Berek JS, Matias-Guiu X, Creutzberg C, Fotopoulou C, Gaffney D, Kehoe S. (2023). "FIGO staging of endometrial cancer: 2023.". Int J Gynaecol Obstet.
- McCluggage WG, Bosse T, Gilks CB, Howitt BE, McAlpine JN, Nucci MR. (2023). "FIGO 2023 endometrial cancer staging: too much, too soon?". Int J Gynecol Cancer.
- (January 1980). "Stage Information for Endometrial Cancer". [[National Cancer Institute]].
- (2021). "StatPearls [Internet]". StatPearls Publishing.
- "Protocol for the Examination of Specimens From Patients With Carcinoma and Carcinosarcoma of the Endometrium, Version: 5.0.0.0".
- (October 2018). "Laparoscopy versus laparotomy for the management of early stage endometrial cancer". The Cochrane Database of Systematic Reviews.
- (2012). "Williams Gynecology". [[McGraw-Hill]].
- (2012). "Williams Gynecology". [[McGraw-Hill]].
- (2013). "Comprehensive Gynecology". [[Mosby (publisher).
- (2013). "Comprehensive Gynecology". [[Mosby (publisher).
- (November 2014). "Exploiting DNA mismatch repair deficiency as a therapeutic strategy". Experimental Cell Research.
- (October 2019). "PI3K/AKT/mTOR inhibitors for advanced or recurrent endometrial cancer". The Cochrane Database of Systematic Reviews.
- (June 2011). "Adjuvant progestagens for endometrial cancer". The Cochrane Database of Systematic Reviews.
- (December 2010). "Hormonal therapy in advanced or recurrent endometrial cancer". The Cochrane Database of Systematic Reviews.
- (March 2006). "Endometrial cancer risk was lower in women who used continuous combined HRT than in non-users". Evidence-based Obstetrics & Gynecology.
- (22 April 2021). "FDA Approves Immunotherapy for Endometrial Cancer with Specific Biomarker". [[FDA]].
- (2 March 2014). "Survival by stage of endometrial cancer". [[American Cancer Society]].
- (May 2013). "Follow-up practice in endometrial cancer and the association with patient and hospital characteristics: a study from the population-based PROFILES registry". Gynecologic Oncology.
- (February 2014). "Exenterative surgery for recurrent gynaecological malignancies". The Cochrane Database of Systematic Reviews.
- (2013). "Comprehensive Gynecology". [[Mosby (publisher).
- (July 2009). "Endometrial cancer and obesity: epidemiology, biomarkers, prevention and survivorship". Gynecologic Oncology.
- (June 2015). "Obesity, diet, physical activity, and health-related quality of life in endometrial cancer survivors". Nutrition Reviews.
- (2013). "Comprehensive Gynecology". [[Mosby (publisher).
- (23 April 2014). "General Information about Endometrial Cancer". NIH.
- (August 2014). "Endometrial cancer: a review and current management strategies: part I". Gynecologic Oncology.
- (October 2013). "The Role of PARP Inhibitors in the Treatment of Gynecologic Malignancies". Frontiers in Oncology.
- (January 2014). "PARP Inhibitors for BRCA1/2 mutation-associated and BRCA-like malignancies". Annals of Oncology.
- (December 2011). "PARP inhibitors in BRCA gene-mutated ovarian cancer and beyond". Current Oncology Reports.
- (July 2014). "Major clinical research advances in gynecologic cancer in 2013". Journal of Gynecologic Oncology.
- (2014). "Metformin in reproductive health, pregnancy and gynaecological cancer: established and emerging indications". Human Reproduction Update.
- (March 2011). "Progestin intrauterine device and GnRH analogue for uterus-sparing treatment of endometrial precancers and well-differentiated early endometrial carcinoma in young women". Annals of Oncology.
- (January 2018). "Treatment of Low-Risk Endometrial Cancer and Complex Atypical Hyperplasia With the Levonorgestrel-Releasing Intrauterine Device". Obstetrics and Gynecology.
- (18 June 2014). "Womb cancer research". Cancer Research UK.
- (2020-11-12). "Womb cancer could be detected early with an inexpensive new blood test". NIHR Evidence.
- (May 2020). "Detecting Endometrial Cancer by Blood Spectroscopy: A Diagnostic Cross-Sectional Study". Cancers.
- (March 2023). "Interventions for weight reduction in obesity to improve survival in women with endometrial cancer". The Cochrane Database of Systematic Reviews.
- (21 September 2014). "Womb cancer: the most common diagnosis you've never heard of". The Guardian.
This article was imported from Wikipedia and is available under the Creative Commons Attribution-ShareAlike 4.0 License. Content has been adapted to SurfDoc format. Original contributors can be found on the article history page.
Ask Mako anything about Endometrial cancer — get instant answers, deeper analysis, and related topics.
Research with MakoFree with your Surf account
Create a free account to save articles, ask Mako questions, and organize your research.
Sign up freeThis content may have been generated or modified by AI. CloudSurf Software LLC is not responsible for the accuracy, completeness, or reliability of AI-generated content. Always verify important information from primary sources.
Report