From Surf Wiki (app.surf) — the open knowledge base
Adrenocortical carcinoma
Cancer of the adrenal cortex

Cancer of the adrenal cortex
| Field | Value |
|---|---|
| name | Adrenocortical carcinoma |
| synonyms | Adrenal cortical carcinoma, adrenocorticocarcinoma, adrenal cortical cancer, adrenal cortex cancer |
| image | Adrenal cortical carcinoma - low mag.jpg |
| caption | Micrograph of an adrenocortical carcinoma (left of image – dark blue) and the adrenal cortex it arose from (right-top of image – pink/light blue). Benign adrenal medulla is present (right-middle of image – gray/blue). H&E stain. |
| field | Oncology |
Adrenocortical carcinoma (ACC) is an aggressive cancer originating in the cortex (steroid hormone-producing tissue) of the adrenal gland.
Adrenocortical carcinoma is remarkable for the many hormonal syndromes that can occur in patients with steroid hormone-producing ("functional") tumors, including Cushing's syndrome, Conn syndrome, virilization, and feminization. Adrenocortical carcinoma has often invaded nearby tissues or metastasized to distant organs at the time of diagnosis, and the overall 5-year survival rate is about 50%.
Adrenocortical carcinoma is a rare tumor, with incidence of one to two per million population annually. It has a bimodal distribution by age, with cases clustering in children under 5 and in adults 30–40 years old. The widely used angiotensin-II-responsive steroid-producing cell line H295R was originally isolated from a tumor diagnosed as adrenocortical carcinoma.
Adrenocortical carcinoma can occur at any age, with the highest incidence between 40 and 60 years of age. Women are more frequently affected (55 to 60%) than men (40 to 45%). Adrenocortical carcinomas usually occur sporadically in adults. However, they sometimes occur as part of hereditary syndromes, such as:
- Li-Fraumeni syndrome
- Lynch syndrome
- Multiple endocrine neoplasia (MEN)
- Familial adenomatous polyposis (see also adenomatosis)
Signs and symptoms
Adrenocortical carcinoma may present differently in children and adults. Most tumors in children are functional, and virilization is by far the most common presenting symptom(s), followed by Cushing's syndrome and precocious puberty. Among adults presenting with hormonal syndromes, Cushing's syndrome alone is most common, followed by mixed Cushing's and virilization (glucocorticoid and androgen overproduction). Feminization and Conn syndrome (mineralocorticoid excess) occur in less than 10% of cases. Rarely, pheochromocytoma-like hypersecretion of catecholamines has been reported in adrenocortical cancers. Nonfunctional tumors (about 40%, authorities vary) usually present with abdominal or flank pain, varicocele, and renal vein thrombosis or they may be asymptomatic and detected incidentally.
All patients with suspected ACC should be carefully evaluated for signs and symptoms of hormonal syndromes. For Cushing's syndrome (glucocorticoid excess), these include weight gain, muscle wasting, purple lines on the abdomen, a fatty "buffalo hump" on the neck, a "moon-like" face, and thinning, fragile skin. Virilism (androgen excess) is most obvious in women, and may produce excess facial and body hair, acne, enlargement of the clitoris, deepening of the voice, coarsening of facial features, cessation of menstruation. Conn syndrome (mineralcorticoid excess) is marked by high blood pressure, which can result in headache and hypokalemia (low serum potassium, which can in turn produce muscle weakness, confusion, and palpitations), low plasma renin activity, and high serum aldosterone. Feminization (estrogen excess) is most readily noted in men, and includes breast enlargement, decreased libido, and impotence.
Pathophysiology
The main etiologic factor of ACC is unknown, although families with Li–Fraumeni syndrome, caused by an inherited inactivation mutation in TP53, have increased risk. Several genes have been shown to be recurrently mutated, including TP53, CTNNB1, MEN1, PRKAR1A, RPL22, and DAXX. The telomerase gene TERT is often amplified while ZNRF3 and CDKN2A are often homozygously deleted. The genes h19, insulin-like growth factor II (IGF-II), and p57kip2 are important for fetal growth and development. They are located on chromosome 11p. Expression of the h19 gene is markedly reduced in both nonfunctioning and functioning adrenal cortical carcinomas, especially in tumors producing cortisol and aldosterone. Also, a loss occurs of activity of the p57kip2 gene product in virilizing adenomas and adrenal cortical carcinomas. In contrast, *IGF-II gene expression has been shown to be high in adrenal cortical carcinomas. Finally, c-myc *gene expression is relatively high in neoplasms, and it is often linked to poor prognosis.
Bilateral adrenocortical tumors are less common than unilateral. The majority of bilateral tumours can be distinguished according to size and aspect of the nodules: primary pigmented nodular adrenocortical disease, which can be sporadic or part of Carney complex, and primary bilateral macro nodular adrenal hyperplasia.Metastasis is most commonly to the liver and lung.
Diagnosis
Incidental discovery
Approximately 30% of adrenal gland carcinomas are diagnosed incidentally (incidentalomas). However, the probability that an adrenal gland incidentaloma is a carcinoma of the adrenal cortex is very low. Adenomas are much more common in this situation. Other benign or malignant tumors can also be the underlying cause.
Laboratory findings
Hormonal syndromes should be confirmed with laboratory testing. Laboratory findings in Cushing syndrome include increased serum glucose (blood sugar) and increased urine cortisol. Adrenal virilism is confirmed by the finding of an excess of serum androstenedione and dehydroepiandrosterone. Findings in Conn syndrome include low serum potassium, low plasma renin activity, and high serum aldosterone. Feminization is confirmed with the finding of excess serum estrogen.
Imaging
Radiological studies of the abdomen, such as CT scans and magnetic resonance imaging are useful for identifying the site of the tumor, differentiating it from other diseases, such as adrenocortical adenoma, and determining the extent of invasion of the tumor into surrounding organs and tissues. On CT, it shows heterogeneous appearance due to necrosis, calcifications, and haemorrhage. After contrast injection, it shows peripheral enhancement. Invasion of adjacent structures such as kidney, vena cava, liver, and retroperitoneal lymph nodes are also common. Online open-access datasets of adrenocortical carcinoma CT examinations are available.
On MRI, it shows low intensity on T1-weighted images, and high T2 signal with strong heterogeneous contrast enhancement and slow washout. Haemorrhagic areas may show high T1-signal. Imaging with positron emission tomography (PET) is useful during initial investigation of potentially malignant adrenal tumors and for detecting metastasis. Fluorodeoxyglucose ([18F]FDG or FDG) has high sensitivity but cannot distinguish ACC from other malignancies. 11C-labelled metomidate binds to enzymes expressed in adrenocortical cells and has been used as a radiotracer with high specificity for adrenal tumors.
Pathology
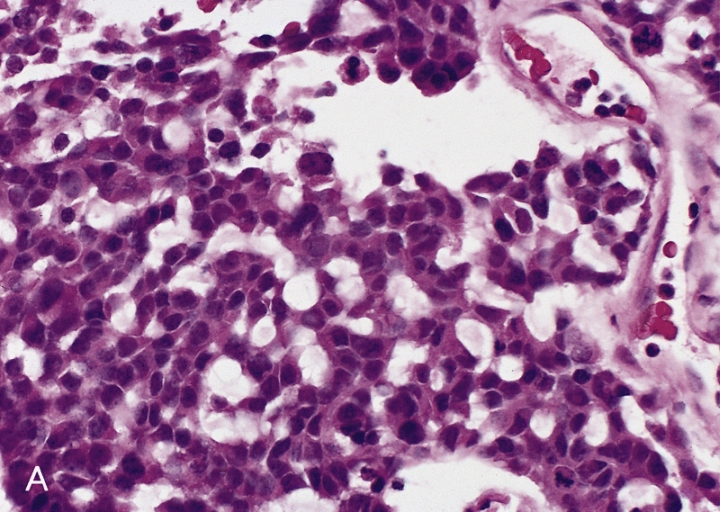
Adrenal tumors are often not biopsied prior to surgery, so diagnosis is confirmed on examination of the surgical specimen by a pathologist. Grossly, ACCs are often large, with a tan-yellow cut surface, and areas of hemorrhage and necrosis. On microscopic examination, the tumor usually displays sheets of atypical cells with some resemblance to the cells of the normal adrenal cortex. The presence of invasion and mitotic activity help differentiate small cancers from adrenocortical adenomas. Several relatively rare variants of ACC include:
- Oncocytic adrenal cortical carcinoma
- Myxoid adrenal cortical carcinoma
- Carcinosarcoma
- Adenosquamous adrenocortical carcinoma
- Clear cell adrenal cortical carcinoma
Differential diagnosis
Differential diagnosis includes:
- Adrenocortical adenoma
- Renal cell carcinoma
- Pheochromocytoma
- Hepatocellular carcinoma
Adrenocortical carcinomas are most commonly distinguished from adrenocortical adenomas (their benign counterparts) by the Weiss system, as follows:
| Characteristic | Score |
|---|---|
| High nuclear grade (enlarged, oval to lobated, with coarsely granular to hyperchromatic chromatin and easily discernible, prominent nucleoli) | 1 |
| More mitoses than 5/50 high power fields | 1 |
| Atypical mitoses | 1 |
| Eosinophilic cytoplasm in 75% of tumor cells | 1 |
| Diffuse architecture of 33% of tumor | 1 |
| Necrosis | 1 |
| Venous invasion | 1 |
| Sinusoidal invasion (no smooth muscle in wall) | 1 |
| Capsular invasion | 1 |
Total score indicates:
- 0-2: Adrenocortical adenoma
- 3: Undetermined
- 4-9: Adrenocortical carcinoma
Prognosis
ACC, generally, carries a poor prognosis, with an overall 5-year survival rate of about 50%. Five-year disease-free survival for a complete resection of a stage I–III ACC is about 30%. The most important prognostic factors are age of the patient and stage of the tumor. Poor prognostic factors include mitotic activity, venous invasion, weight of 50 g or more, diameter of 6.5 cm or more, Ki-67/MIB1 labeling index of 4% or more, and p53 positive.
In its malignancy, adrenocortical carcinoma is unlike most tumours of the adrenal cortex, which are benign (adenomas) and only occasionally cause Cushing's syndrome.
Treatment
The only curative treatment is complete surgical excision of the tumor, which can be performed even in the case of invasion into large blood vessels, such as the renal vein or inferior vena cava. The 5-year survival rate after successful surgery is 50–60%, but unfortunately, many patients are not surgical candidates. A 2018 systematic review suggests that laparoscopic retroperotenial adrenalectomy appears to reduce late morbidity, time to oral fluid or food intake and time to ambulation when compared to laparoscopic transperitoneal adrenalectomy, however there is uncertainty about these effects due to very low-quality evidence. For outcomes such as all-cause mortality, early morbidity, socioeconomic effects, and operative and postoperative parameter, the evidence is uncertain about the effects of either interventions over the other.
Radiation therapy and radiofrequency ablation may be used for palliation in patients who are not surgical candidates. Minimally invasive surgical techniques remain controversial due to the absence of long-term data, with a particular concern for rates of recurrence and peritoneal carcinomatosis.
Chemotherapy regimens typically include the drug mitotane, an inhibitor of steroid synthesis, which is toxic to cells of the adrenal cortex, as well as standard cytotoxic drugs. A retrospective analysis showed a survival benefit for mitotane in addition to surgery when compared to surgery alone.
The two most common regimens are cisplatin, doxorubicin, etoposide (EDP) + mitotane, and streptozotocin + mitotane. The FIRM-ACT trial demonstrated higher rates of response and longer progression-free survival with EDP + mitotane than with streptozotocin + mitotane.
Therapy studies
Due to the rarity of the disease, many important questions about adrenocortical carcinoma remain unanswered. Therefore, as many patients as possible should be treated in registry studies or therapy studies.
Therapy support
In addition to therapy primarily focused on treating the tumor, the treating physician will administer supportive therapy. Furthermore, there are numerous other support services available. These can help patients and their families cope better with the diagnosis, cancer treatment, and the consequences of the disease. The following list is not a complete overview of all available support services. It consists of examples that can facilitate the initial search for suitable support for the individual patient.
- Genetic counseling
- Pregnancy and adrenocortical carcinoma
- Advice centers, general
- Advice centers, special topics
- Other assistance
- Self-help groups (e.g. LET'S CURE ACC, https://letscureacc.com/)
Children with adrenocotrical carcinoma
General information
Adrenocortical carcinoma is extremely rare in children (approximately 0.2 to 0.3 cases per 1 million per year). The prognosis is poor. There are currently no established standards for diagnosis and treatment. Therefore, the "ENSAT kids" study group was established for children with adrenocortical carcinoma within ENSAT. While only a proportion of adrenocortical carcinomas in adults are hormonally active, almost all of these carcinomas are hormonally active in affected children. Cushing's syndrome, precocious puberty, or virilization usually occur. As with the treatment of adult patients, the tumor is completely removed surgically. If an advanced stage is present, lymph nodes are also removed in children, and chemotherapy and mitotane therapy are administered.
State of research
Approximately 70% of affected children are female. Of these, about 90% are hormone-active carcinomas.
- 50% androgens
- 30% mixed
- 10% steroids
- 10% hormone-inactive The average time from the onset of symptoms to diagnosis is six months. Approximately 70% of tumors can be completely removed surgically.
The current state of research is considered insufficient. The few available comparisons between adrenocortical carcinomas in adults and children indicate significant differences. Therefore, findings obtained so far in adults cannot be readily applied to children. To close these knowledge gaps and to be able to determine suitable therapies for children, a better molecular biological understanding of the prognosis and tumor biology of adrenocortical tumors in children is needed.
Currently, the main research questions are:
- Clinical: International assessment of diagnostics and therapy with the aim of improving clinical understanding and treatment procedures.
- Clinical-translational: Analysis of the significance of plasma and urine steroid profiles / liquid biopsy with the aim of identifying suitable tumor markers.
- Experimental: Identification of immunohistochemical characteristics and DNA sequencing with the aim of identifying drugable targets, i.e., targets for the drug treatment of tumor cells. This should ensure that healthy cells are spared from the drug as much as possible.
References
References
- (25 June 2012). "Adrenal Gland Tumor: Statistics".
- (October 2018). "European Society of Endocrinology Clinical Practice Guidelines on the management of adrenocortical carcinoma in adults, in collaboration with the European Network for the Study of Adrenal Tumors". European Journal of Endocrinology.
- (June 2012). "Combination chemotherapy in advanced adrenocortical carcinoma". The New England Journal of Medicine.
- (2005). "Cancer: principles & practice of oncology". Lippincott-Raven.
- (2006-08-08). "Clinical presentation and evaluation of adrenocortical tumors". UpToDate.
- (March 2012). "Human adrenocortical carcinoma cell lines". Molecular and Cellular Endocrinology.
- (September 1990). "Establishment and characterization of a human adrenocortical carcinoma cell line that expresses multiple pathways of steroid biosynthesis". Cancer Research.
- Martin Fassnacht, Olaf Dekkers, Tobias Else, Eric Baudin, Alfredo Berruti, Ronald. R. de Krijger, Harm R. Haak, Radu Mihai, Guillaume Assie, Massimo Terzolo: European Society of Endocrinology clinical practice guidelines on the management of adrenal incidentalomas, in collaboration with the European Network for the Study of Adrenal Tumors. In: European Journal of Endocrinology. Volume 179, Issue 4, October 2018, Pages G1–G46, https://doi.org/10.1530/EJE-18-0608 [retrieved November 10, 2024]
- (August 2011). "Adrenocortical carcinoma presenting as varicocele and renal vein thrombosis: a case report". Journal of Medical Case Reports.
- Kasper DL, Braunwald E, Fauci AS, Hauser SL, Longo DL, Jameson JL. ''Harrison's Principles of Internal Medicine''. New York: McGraw-Hill, 2005. {{ISBN. 0-07-139140-1
- (May 2016). "Comprehensive Pan-Genomic Characterization of Adrenocortical Carcinoma". Cancer Cell.
- (June 2014). "Integrated genomic characterization of adrenocortical carcinoma". Nature Genetics.
- (2000). "Cancer medicine". B.C. Decker.
- James Norman. (16 February 2023). "Diseases of the Adrenal Cortex: Adrenal Cancer".
- (January 2019). "Imaging features of adrenal masses". Insights into Imaging.
- "Adrenal-ACC-Ki67-Seg: Adrenocortical Carcinoma".
- "ADRENAL-ACC-KI67-SEG".
- (August 2016). "Molecular Imaging in the Management of Adrenocortical Cancer: A Systematic Review". Clinical Nuclear Medicine.
- (November 2016). "Targeted Molecular Imaging in Adrenal Disease-An Emerging Role for Metomidate PET-CT". Diagnostics.
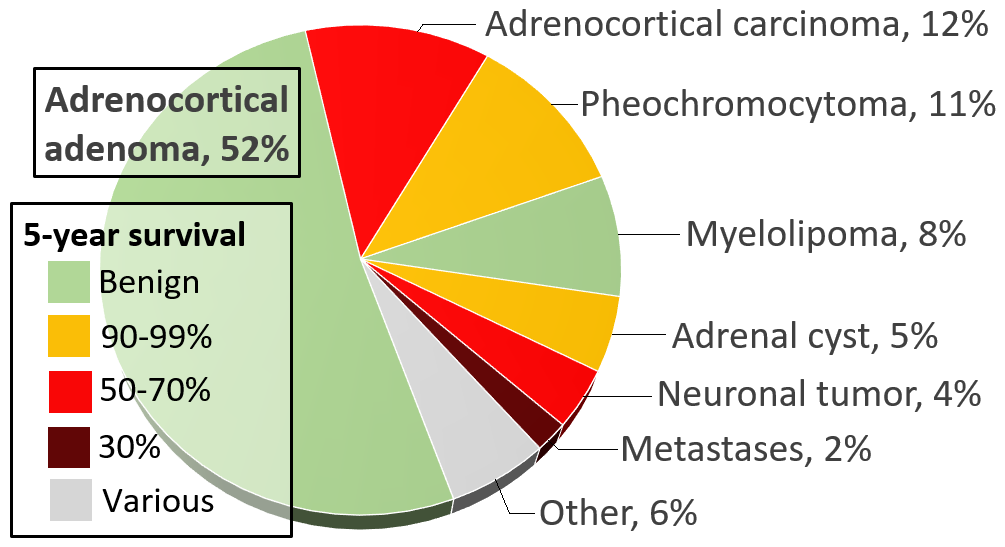
- Data and references for pie chart are located at [[Commons:File:Incidences and prognoses of adrenal tumors.png. file description page in Wikimedia Commons.]]
- (March 2014). "Distinguishing adrenal cortical carcinomas and adenomas: a study of clinicopathological features and biomarkers". Histopathology.
- (2015). "Adrenocortical Oncocytoma Presenting with Gynaecomastia". Journal of the ASEAN Federation of Endocrine Societies.
- (26 December 2016). "Adrenocortical Cancer".
- (June 2006). "Clinical review: Adrenocortical carcinoma: clinical update". The Journal of Clinical Endocrinology and Metabolism.
- (December 2018). "Transperitoneal versus retroperitoneal laparoscopic adrenalectomy for adrenal tumours in adults". The Cochrane Database of Systematic Reviews.
- (2006). "Goodman & Gilman's The Pharmacological Basis of Therapeutics". The McGraw-Hill Companies, Inc..
- (June 2007). "Adjuvant mitotane treatment for adrenocortical carcinoma". The New England Journal of Medicine.
- (June 2012). "Combination chemotherapy in advanced adrenocortical carcinoma". The New England Journal of Medicine.
- [https://www.ukw.de/kinderklinik/forschung/nebennierenkarzinome/ Pediatric adrenal carcinomas (deutsch, Pädiatrische Nebennierenkarzinome], at ukw.de, retrieved July 13, 2024
- Maria Riedmeier, Boris Decarolis, Imme Haubitz, Sophie Müller, Konstantin Uttinger, Kevin Börner, Joachim Reibetanz, Armin Wiegering, Christoph Härtel, Paul-Gerhardt Schlegel, Martin Fassnacht and Verena Wiegering: Adrenocortical Carcinoma in Childhood: A Systematic Review. In: MDPI Cancers 2021, 13(21), published: 20 October 2021. 5266. https://www.doi.org//10.3390/cancers13215266 [retrieved July 15, 2024]
- [https://www.glandula-online.de/fileadmin/user_upload/Aktuelle_Meldungen/GLANDUlinchen_2-22.pdf/ Actual Item at GLANDUlinchen (deutsch, Aktuelle Meldungen in GLANDUlinchen], at ukw.de, retrieved August 4, 2024
This article was imported from Wikipedia and is available under the Creative Commons Attribution-ShareAlike 4.0 License. Content has been adapted to SurfDoc format. Original contributors can be found on the article history page.
Ask Mako anything about Adrenocortical carcinoma — get instant answers, deeper analysis, and related topics.
Research with MakoFree with your Surf account
Create a free account to save articles, ask Mako questions, and organize your research.
Sign up freeThis content may have been generated or modified by AI. CloudSurf Software LLC is not responsible for the accuracy, completeness, or reliability of AI-generated content. Always verify important information from primary sources.
Report